Aflac Ub04 Form
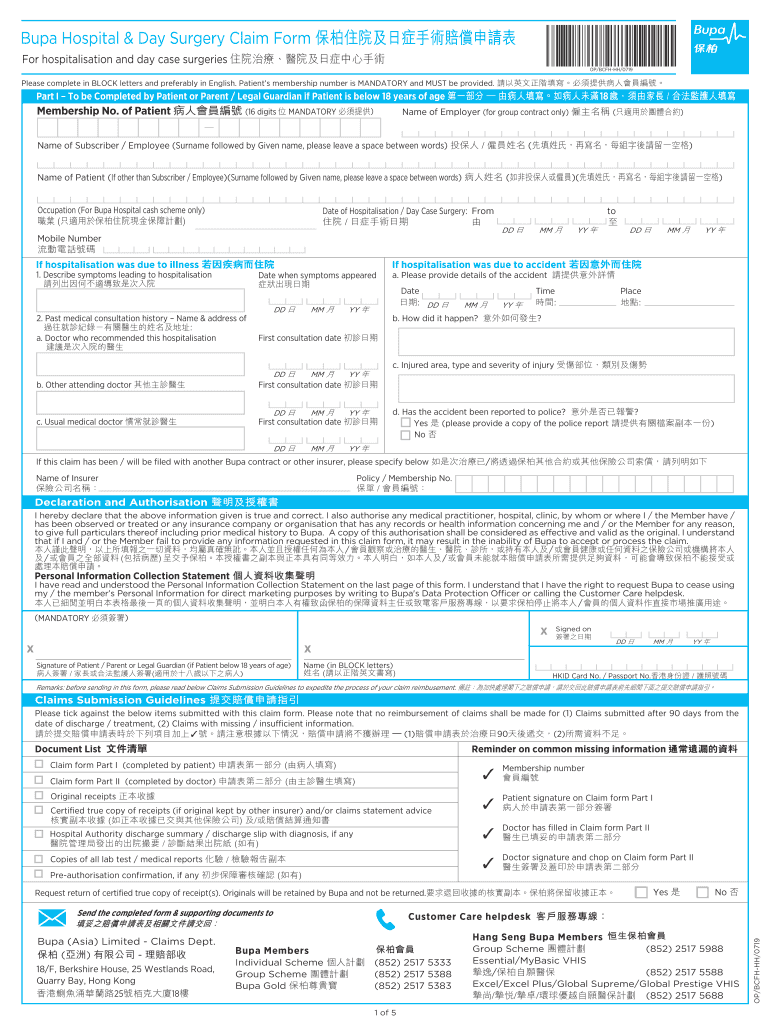
Aflac Ub04 Form - Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Policyholder information (please print.) first name initial last name mailing address city statezip check box if this is anew permanent address: We are providing two different versions in case one works better for you than the other. Complete policyholder/patient information and sign your claim form. Date of injury or when symptoms first occurred.physician’s name, address and phone/fax number. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy). Web hospital indemnity claim form instructions. This * denotes a required field. Supporting documentation needed itemized bill if there was a hospital stay (ub04 from the hospital or medical facility) Definitions & acronyms emergency room (er).
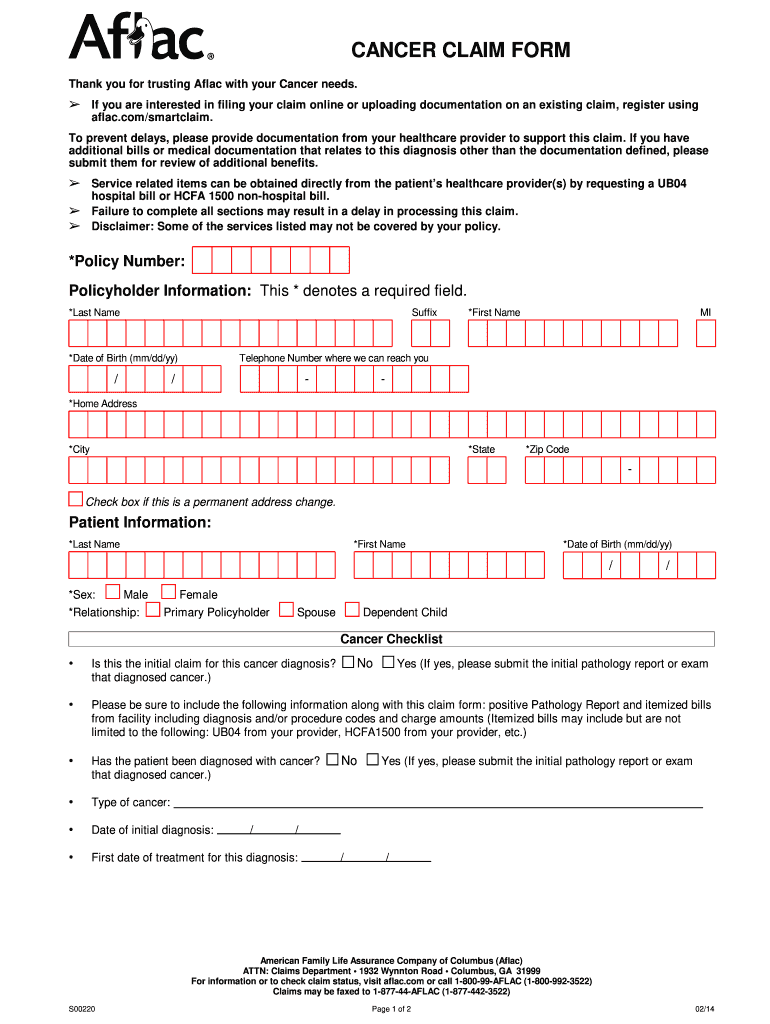
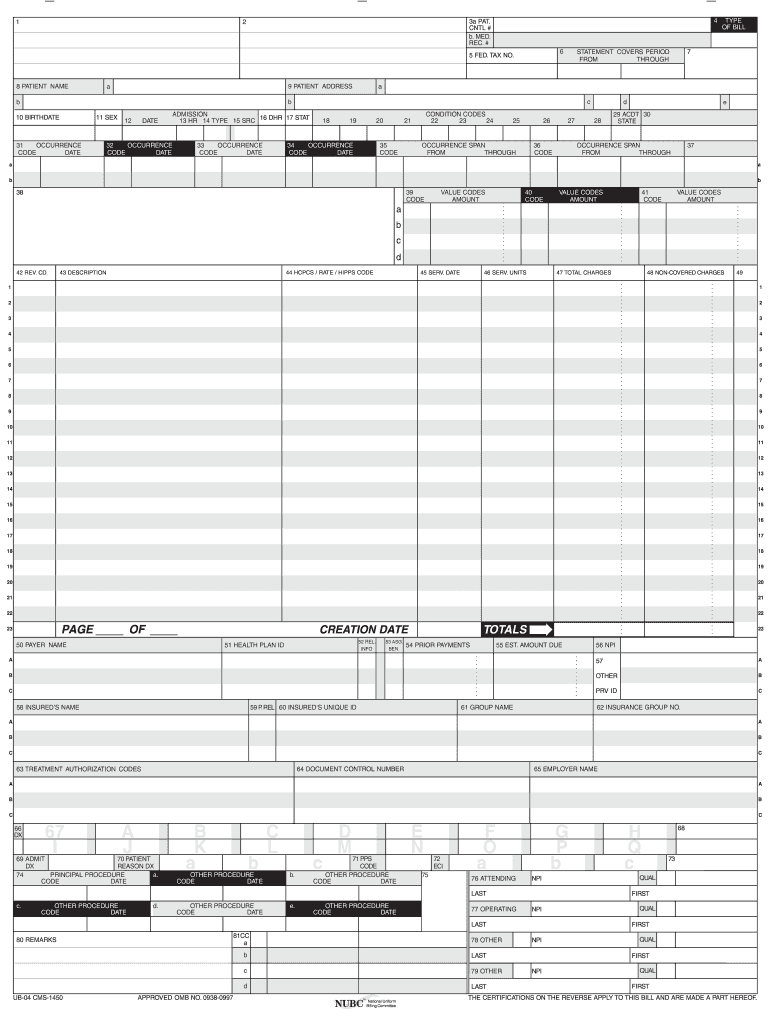
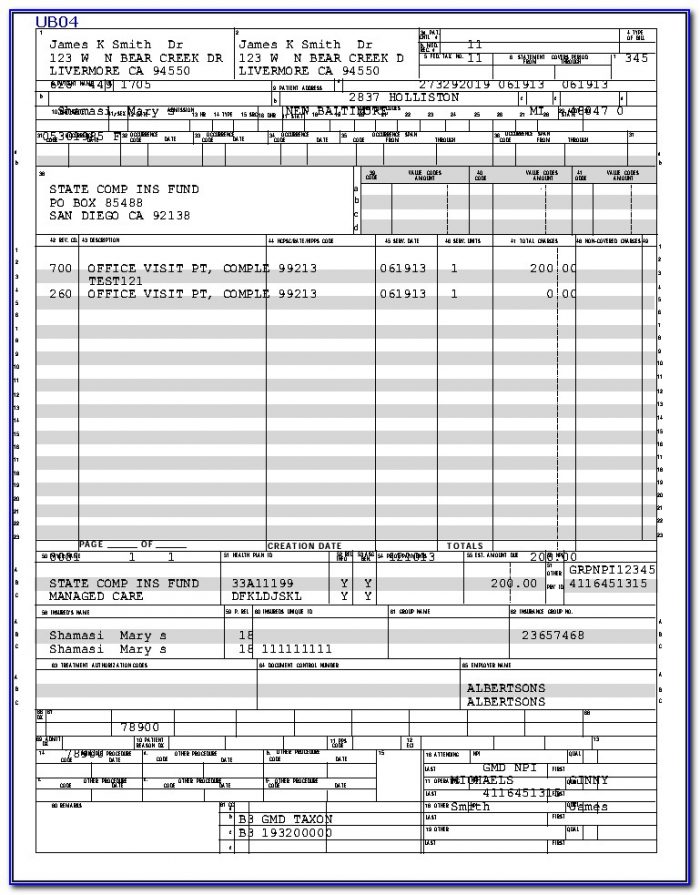
We are providing two different versions in case one works better for you than the other. To avoid delays in processing of your claim form, complete each section attaching documentation below whenit applies. Web what you need to file a claim patient’s name and date of birth.patient’s relationship to policyholder. Policyholder information (please print.) first name initial last name mailing address city statezip check box if this is anew permanent address: Definitions & acronyms emergency room (er). Physician billing is done on the cms 1500 claim forms. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy). Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Complete policyholder/patient information and sign your claim form. This * denotes a required field.
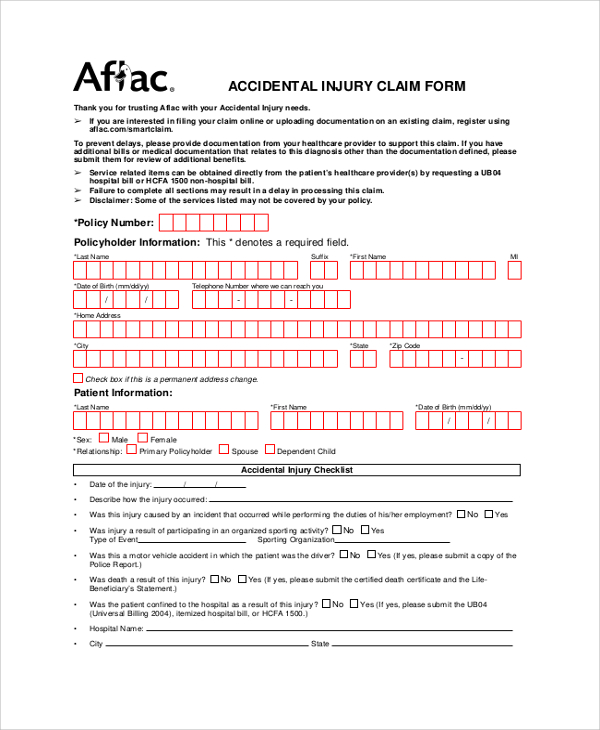
Complete policyholder/patient information and sign your claim form. To avoid delays in processing of your claim form, complete each section attaching documentation below whenit applies. Definitions & acronyms emergency room (er). *last name suffix *first name mi *date of birth (mm/dd/yy) Aflac accident injury claim form accidental injury claim form failure to complete this form in its entirety may result in a delay in processing this claim. Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to bill their services on the ub04 form in order to get paid. Physician billing is done on the cms 1500 claim forms. Web hospital indemnity claim form instructions. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy). Web ub 04 form aflac.
Hospital Claim Form 20190719 Fill Out and Sign Printable PDF Template
Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. This * denotes a required field. *last name suffix *first name mi *date of birth (mm/dd/yy) Web hospital indemnity claim form instructions. Have the treating physician complete section b:.
Aflac Claim Forms Printable Master of Documents
This * denotes a required field. To avoid delays in processing of your claim form, complete each section attaching documentation below whenit applies. Date of injury or when symptoms first occurred.physician’s name, address and phone/fax number. Policyholder information (please print.) first name initial last name mailing address city statezip check box if this is anew permanent address: Have the treating.
Aflac Wellness Claim Forms Printable Customize and Print
Web what you need to file a claim patient’s name and date of birth.patient’s relationship to policyholder. Have the treating physician complete section b:. Our customer service representatives are here to assist you monday. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to.
Ub04 Form Fill Online, Printable, Fillable, Blank pdfFiller
Our customer service representatives are here to assist you monday. Physician billing is done on the cms 1500 claim forms. Web ub 04 form aflac. We are providing two different versions in case one works better for you than the other. Have the treating physician complete section b:.

6 Ub 04 form Template FabTemplatez
Complete policyholder/patient information and sign your claim form. Web ub 04 form aflac. Physician billing is done on the cms 1500 claim forms. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy).

6 Ub 04 form Template FabTemplatez
Complete policyholder/patient information and sign your claim form. Policyholder information (please print.) first name initial last name mailing address city statezip check box if this is anew permanent address: Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Web ub 04 form aflac. Definitions & acronyms emergency room (er).
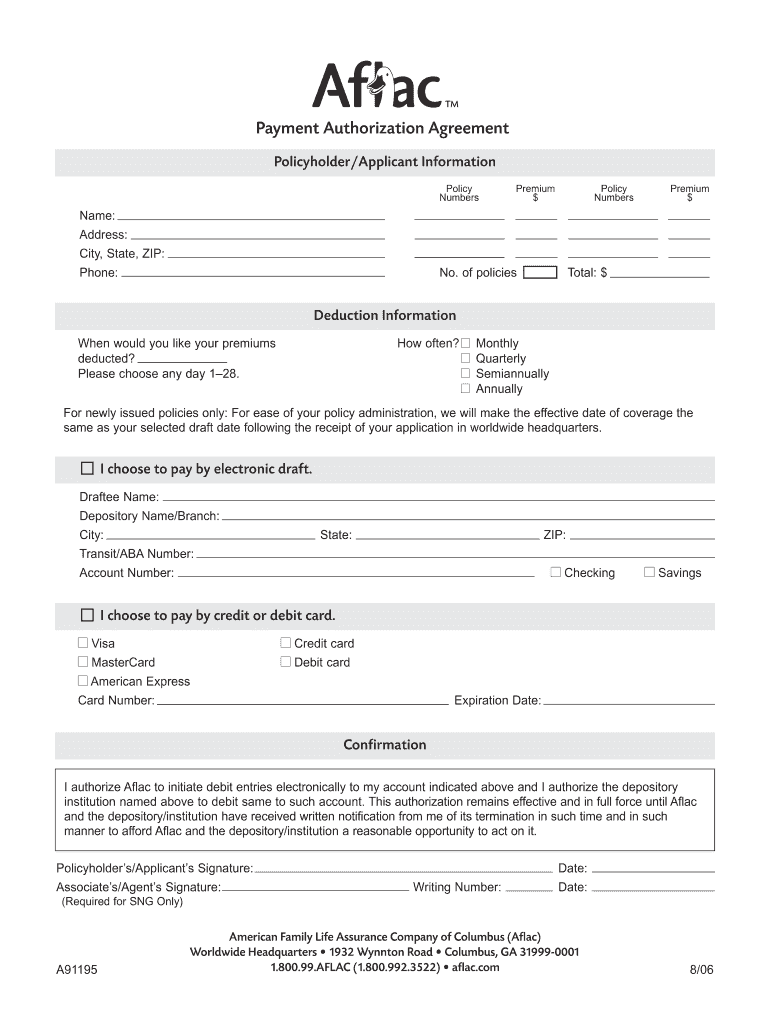
Payment Authorization Agreement Fill Out and Sign Printable PDF
Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Web hospital indemnity claim form instructions. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. *last name suffix *first name mi *date of birth (mm/dd/yy).
Blank Ub 04 Claim Form Form Resume Examples rykgPYKDwn
Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to bill their services on the ub04 form in order to get paid. Web what you need to file a claim patient’s name and date of birth.patient’s relationship to policyholder. Web ub 04 form aflac. Date of injury or when symptoms first occurred.physician’s name, address and phone/fax number. Complete policyholder/patient information.

6 Ub 04 form Template FabTemplatez
Aflac accident injury claim form accidental injury claim form failure to complete this form in its entirety may result in a delay in processing this claim. Web what you need to file a claim patient’s name and date of birth.patient’s relationship to policyholder. Date of injury or when symptoms first occurred.physician’s name, address and phone/fax number. *lastname suffix *firstname mi.

CMS1500 and UB04 Forms YouTube
Supporting documentation needed itemized bill if there was a hospital stay (ub04 from the hospital or medical facility) Web hospital indemnity claim form instructions. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy). Our customer service representatives are here to assist you monday. *last name suffix *first name mi *date of birth (mm/dd/yy)
Definitions & Acronyms Emergency Room (Er).
*last name suffix *first name mi *date of birth (mm/dd/yy) Web what you need to file a claim patient’s name and date of birth.patient’s relationship to policyholder. Supporting documentation needed itemized bill if there was a hospital stay (ub04 from the hospital or medical facility) Policyholder information (please print.) first name initial last name mailing address city statezip check box if this is anew permanent address:
Date Of Injury Or When Symptoms First Occurred.physician’s Name, Address And Phone/Fax Number.
This * denotes a required field. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. *lastname suffix *firstname mi *dateofbirth(mm/dd/yy). We are providing two different versions in case one works better for you than the other.
To Avoid Delays In Processing Of Your Claim Form, Complete Each Section Attaching Documentation Below Whenit Applies.
Web ub 04 form aflac. Have the treating physician complete section b:. Physician billing is done on the cms 1500 claim forms. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.
Aflac Accident Injury Claim Form Accidental Injury Claim Form Failure To Complete This Form In Its Entirety May Result In A Delay In Processing This Claim.
Complete policyholder/patient information and sign your claim form. Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to bill their services on the ub04 form in order to get paid. Our customer service representatives are here to assist you monday. Web hospital indemnity claim form instructions.