Ambetter Dispute Form
Ambetter Dispute Form - Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. Web discharge consultation form (pdf) smart goals fact sheet (pdf) claims and claim payment. Mail completed form(s) and attachments to: Web and claim dispute form use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. Web mail completed form(s) and attachments to the appropriate address: Claim complaints must follow the dispute process and then the complaint process below. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Web claim dispute form (pdf) no surprises act open negotiation form (pdf) quality practice guidelines (pdf) hedis quick reference guide (pdf) quality improvement. Medical records may be submitted via the. Web use this form as part of the ambetter from superior healthplan claim dispute process to dispute the decision made during the request for reconsideration.
Payspan (pdf) secure portal (pdf) provider portal enhancements: All fields are required information a request for reconsideration. How do i submit medical records? Web and claim dispute form use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. Claim complaints must follow the dispute process and then the complaint process below. Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. Request for reconsideration po box 5010 farmington,. Web provider complaint/grievance and appeal process. Claim reconsideration and denial explanations (pdf). Web discharge consultation form (pdf) smart goals fact sheet (pdf) claims and claim payment.
1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request. Payspan (pdf) secure portal (pdf) provider portal enhancements: Web use this form as part of the ambetter from superior healthplan claim dispute process to dispute the decision made during the request for reconsideration. Ambetter from silversummit healthplan attn: Ambetter from health net’s appeals and grievances department will oversee the processing of your appeal. Request for reconsideration po box 5010 farmington,. Web discharge consultation form (pdf) smart goals fact sheet (pdf) claims and claim payment. Web and claim dispute form use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. Medical records may be submitted via the. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process.

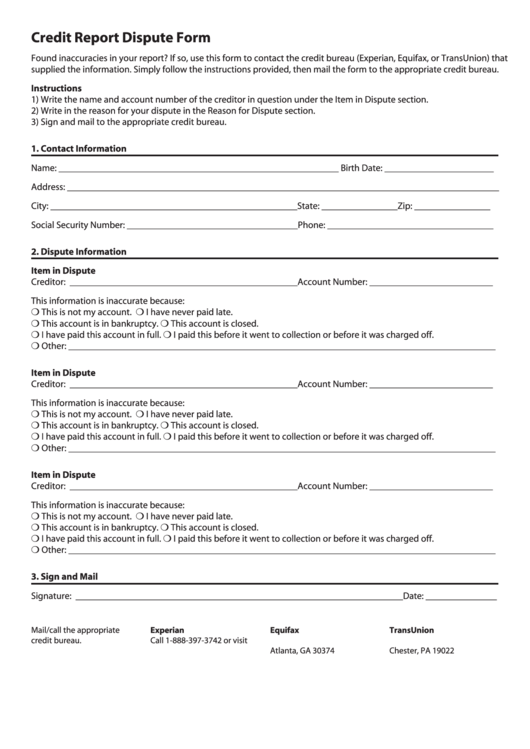
Credit Dispute Form For Experian Form Resume Examples QJ9eXLK2my
Medical records may be submitted via the. Claim complaints must follow the dispute process and then the complaint process below. Web provider complaint/grievance and appeal process. Web and claim dispute form use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. Mail completed form(s) and attachments to:

Universal Credit Dispute Form Letter Experion Equifax Trans Union
Payspan (pdf) secure portal (pdf) provider portal enhancements: All fields are required information a request for reconsideration. Web mail completed form(s) and attachments to the appropriate address: Ambetter from health net’s appeals and grievances department will oversee the processing of your appeal. Use your zip code to find your personal plan.

Dispute Department Fill Online, Printable, Fillable, Blank
Ambetter from silversummit healthplan attn: Medical records may be submitted via the. See coverage in your area; • a claim dispute (level. Request for reconsideration po box 5010 farmington,.
Credit Dispute Form Fill Online, Printable, Fillable, Blank pdfFiller
Web mail completed form(s) and attachments to the appropriate address: How do i submit medical records? Web provider complaint/grievance and appeal process. Claim reconsideration and denial explanations (pdf). No surprises act open negotiation form (pdf) quality.
Arkansas Dispute Resolution Appeal Form Download Fillable PDF
Mail completed form(s) and attachments to: Web and claim dispute form use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. No surprises act open negotiation form (pdf) quality. Claim dispute form (pdf) taxonomy code billing requirement (pdf). Web ambetter claims processing po box 5010.
Huntington Bank ACH Dispute Form 20152022 Fill and Sign Printable
• a claim dispute (level. All fields are required information a request for reconsideration. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Web ambetter claims processing po box 5010. Claim reconsideration and denial explanations (pdf).
Fillable Cardholder Dispute Form Affidavit Of Fraudulent Account
Payspan (pdf) secure portal (pdf) provider portal enhancements: • a claim dispute (level. Use your zip code to find your personal plan. Ambetter from silversummit healthplan attn: Web include this form with a corrected claim.
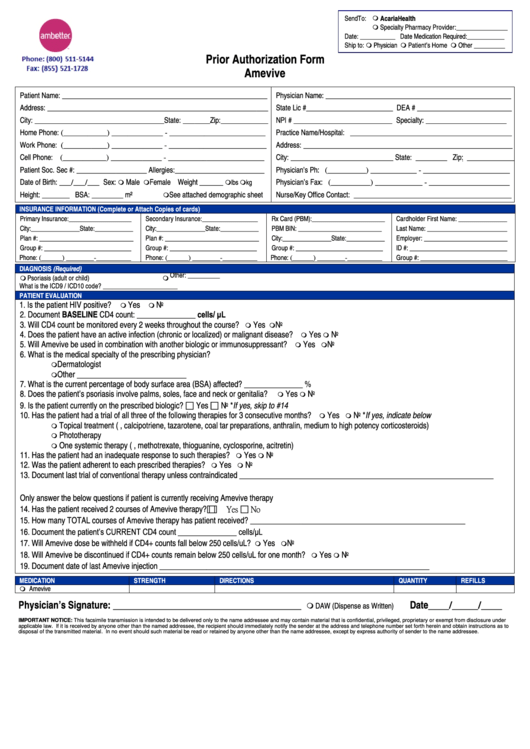
Ambetter Prior Authorization Form Amevive printable pdf download
Web claim dispute form (pdf) no surprises act open negotiation form (pdf) quality practice guidelines (pdf) hedis quick reference guide (pdf) quality improvement. Claim complaints must follow the dispute process and then the complaint process below. Ambetter from silversummit healthplan attn: Claim dispute form (pdf) taxonomy code billing requirement (pdf). Ambetter from health net’s appeals and grievances department will oversee.
Top 7 Equifax Dispute Form Templates free to download in PDF format
Request for reconsideration po box 5010 farmington,. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Ambetter from silversummit healthplan attn: Web claim dispute form (pdf) no surprises act open negotiation form (pdf) quality practice guidelines (pdf) hedis quick reference guide (pdf) quality improvement. Web claim dispute form (pdf) billing and.

What Is The Group Id For Ambetter Https Www Bmc Org Sites Default
Web discharge consultation form (pdf) smart goals fact sheet (pdf) claims and claim payment. Web denial to request a formal appeal. Web a complaint is a written expression by a provider which indicates dissatisfaction or dispute with ambetter's policies, procedure, or any aspect of ambetter's functions. Web use this form as part of the ambetter from sunshine health claim dispute.
All Fields Are Required Information A Request For Reconsideration.
Web include this form with a corrected claim. Web claim dispute form (pdf) no surprises act open negotiation form (pdf) quality practice guidelines (pdf) hedis quick reference guide (pdf) quality improvement. Ambetter from silversummit healthplan attn: Payspan (pdf) secure portal (pdf) provider portal enhancements:
Web Claim Dispute Form (Pdf) Billing And Coding;
Web discharge consultation form (pdf) smart goals fact sheet (pdf) claims and claim payment. Medical records may be submitted via the. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Web use this form as part of the ambetter from superior healthplan claim dispute process to dispute the decision made during the request for reconsideration.
Web Provider Complaint/Grievance And Appeal Process.
Claim reconsideration and denial explanations (pdf). Web ambetter claims processing po box 5010. See coverage in your area; Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed.
Web And Claim Dispute Form Use This Form As Part Of The Ambetter From Home State Health Request For Reconsideration And Claim Dispute Process.
Claim dispute form (pdf) taxonomy code billing requirement (pdf). Web a complaint is a written expression by a provider which indicates dissatisfaction or dispute with ambetter's policies, procedure, or any aspect of ambetter's functions. Mail completed form(s) and attachments to: • a claim dispute (level.