Attending Physician Statement Form
Attending Physician Statement Form - Involved parties names, places of residence and phone numbers etc. Employer information name type of claim Customize the blanks with unique fillable fields. Web get the attending physician statement form you require. Open it up with online editor and start altering. It is written by your doctor, and the information contained in the aps varies and depends on what your insurer is looking for. Web attending physician's statement complete this form in full. Web aps (attending physician statement) is a form required by insurance companies whenever applying for insurance. Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. Web fill online, printable, fillable, blank attending physician statement form.
The form is filled by a physician illustrating the exact medical status of the insured person and if he is suffering any medical condition that conflicts with the insurance plan. Web fill online, printable, fillable, blank attending physician statement form. Customize the blanks with unique fillable fields. Web use this form to provide us with the information we need from you and your physician to process your claim for disability benefits. • you may use the remarks section on the reverse side if you need more room to respond. Involved parties names, places of residence and phone numbers etc. Use fill to complete blank online others pdf forms for free. Open it up with online editor and start altering. Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. It is written by your doctor, and the information contained in the aps varies and depends on what your insurer is looking for.
Involved parties names, places of residence and phone numbers etc. • you may use the remarks section on the reverse side if you need more room to respond. Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. Web an attending physician statement (aps) is a specific report requested by your potential insurer when applying for life insurance coverage or other types of policies. Web fill online, printable, fillable, blank attending physician statement form. Web get the attending physician statement form you require. All forms are printable and downloadable. Web aps (attending physician statement) is a form required by insurance companies whenever applying for insurance. Web use this form to provide us with the information we need from you and your physician to process your claim for disability benefits. Use fill to complete blank online others pdf forms for free.
Attending Physician'S Statement Additional Report Psychological
All forms are printable and downloadable. Web attending physician's statement complete this form in full. Use fill to complete blank online others pdf forms for free. While an aps looks simple, how an aps is completed can make or break your case. The form is filled by a physician illustrating the exact medical status of the insured person and if.
Rbc Attending Physician Supplementary Statement Fill Out and Sign
While an aps looks simple, how an aps is completed can make or break your case. Involved parties names, places of residence and phone numbers etc. Web get the attending physician statement form you require. Once completed you can sign your fillable form or send for signing. Add the day/time and place your electronic signature.

What You Need to Know About Attending Physician Statement Forms
Web attending physician's statement complete this form in full. Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. While an aps looks simple, how an aps is completed can make or break your case. Web use this form to provide us with the information we need from.
ATTENDING PHYSICIAN’S STATEMENT
Involved parties names, places of residence and phone numbers etc. • the patient is responsible for completion of this form without expense to the company. Employer information name type of claim Web aps (attending physician statement) is a form required by insurance companies whenever applying for insurance. While an aps looks simple, how an aps is completed can make or.
Sedgwick Fmla Forms PDF the Form in Seconds Fill Out and Sign
Open it up with online editor and start altering. • you may use the remarks section on the reverse side if you need more room to respond. Use fill to complete blank online others pdf forms for free. While an aps looks simple, how an aps is completed can make or break your case. The form is filled by a.
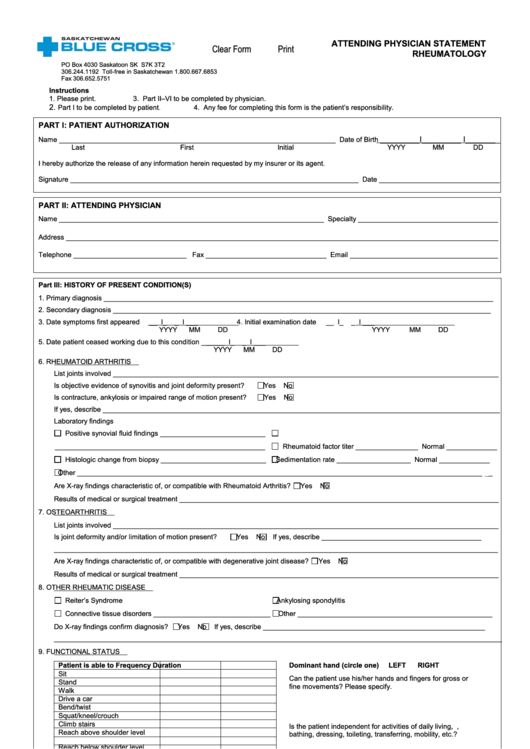
Fillable Rheumatology Attending Physician Statement Form printable pdf
Involved parties names, places of residence and phone numbers etc. Web use this form to provide us with the information we need from you and your physician to process your claim for disability benefits. Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. Add the day/time and.
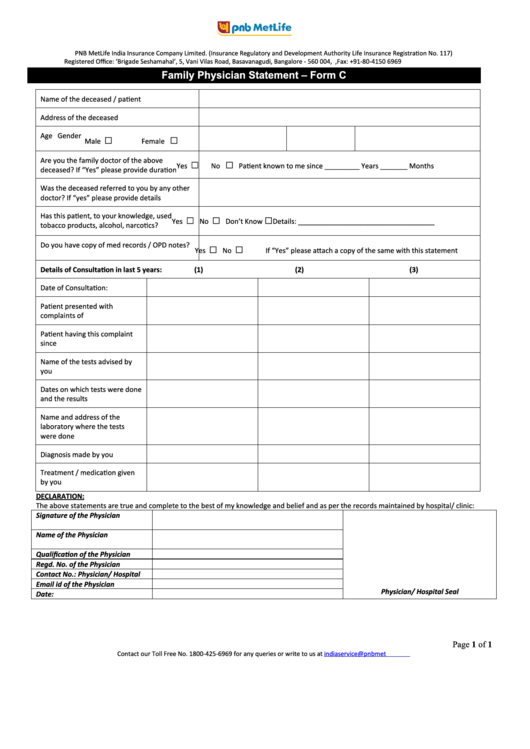
Family Physician Statement Form C printable pdf download
Add the day/time and place your electronic signature. The form is filled by a physician illustrating the exact medical status of the insured person and if he is suffering any medical condition that conflicts with the insurance plan. Web an attending physician statement (aps) is a specific report requested by your potential insurer when applying for life insurance coverage or.
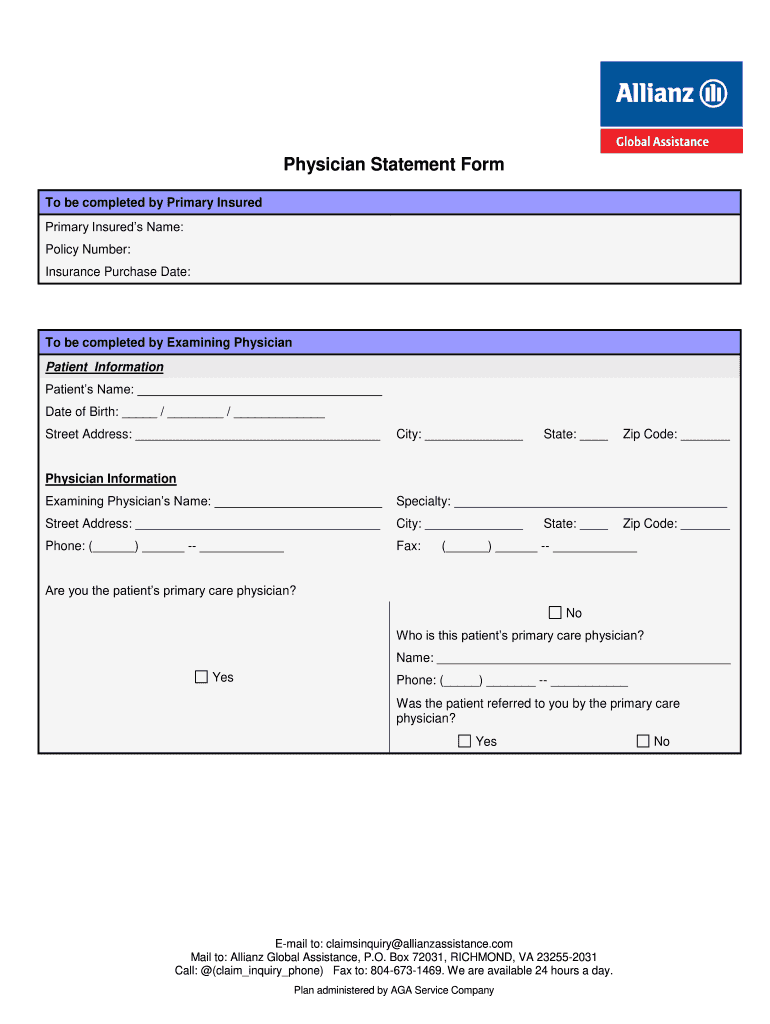
Physician Statement Form Fill Out and Sign Printable PDF Template
Once completed you can sign your fillable form or send for signing. Web aps (attending physician statement) is a form required by insurance companies whenever applying for insurance. Web get the attending physician statement form you require. Metropolitan life insurance company things to know before you begin you should complete and sign section 1 of this form before giving it.
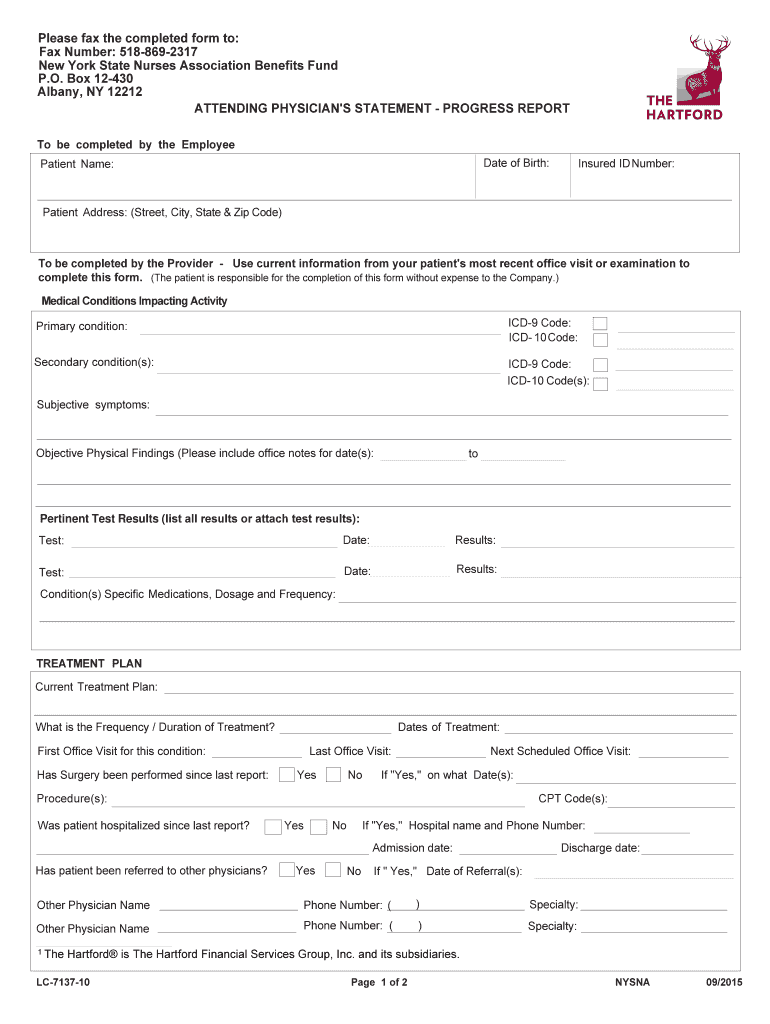
The Hartford Attending Physician Statement Progress Report Fill Out
Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. Use fill to complete blank online others pdf forms for free. Web use this form to provide us with the information we need from you and your physician to process your claim for disability benefits. • the patient.
Insurance Claim FormAttending Physician's Statement
Web attending physician's statement complete this form in full. Web an attending physician statement (aps) is a specific report requested by your potential insurer when applying for life insurance coverage or other types of policies. Employer information name type of claim Web use this form to provide us with the information we need from you and your physician to process.
All Forms Are Printable And Downloadable.
Web an attending physician statement (aps) is a specific report requested by your potential insurer when applying for life insurance coverage or other types of policies. Metropolitan life insurance company things to know before you begin you should complete and sign section 1 of this form before giving it to your physician. While an aps looks simple, how an aps is completed can make or break your case. Web fill online, printable, fillable, blank attending physician statement form.
Involved Parties Names, Places Of Residence And Phone Numbers Etc.
• the patient is responsible for completion of this form without expense to the company. Web use this form to provide us with the information we need from you and your physician to process your claim for disability benefits. The form is filled by a physician illustrating the exact medical status of the insured person and if he is suffering any medical condition that conflicts with the insurance plan. Add the day/time and place your electronic signature.
• You May Use The Remarks Section On The Reverse Side If You Need More Room To Respond.
Patient information name aetna id number birth date (mm/dd/yyyy) gender female male height (ft., in.) weight (lbs.) blood pressure date measured 2. Use fill to complete blank online others pdf forms for free. Open it up with online editor and start altering. Web attending physician's statement complete this form in full.
Web Get The Attending Physician Statement Form You Require.
It is written by your doctor, and the information contained in the aps varies and depends on what your insurer is looking for. Employer information name type of claim Once completed you can sign your fillable form or send for signing. Customize the blanks with unique fillable fields.