Dd Form 2527 Tricare
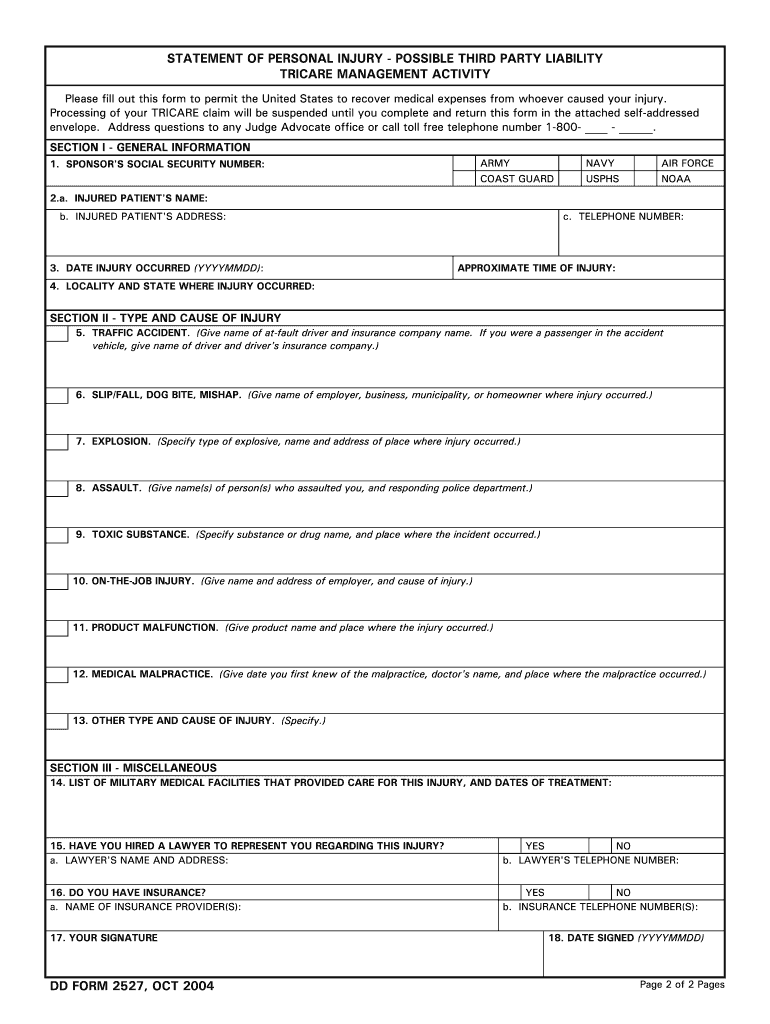
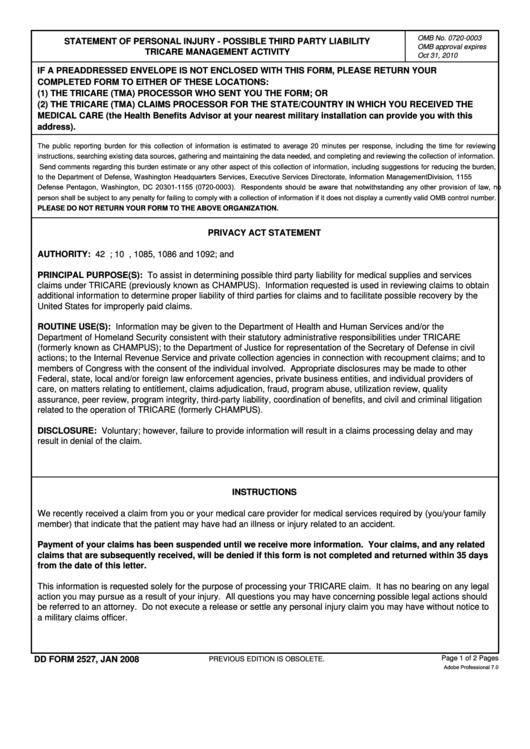
Dd Form 2527 Tricare - Describe condition for which patient received treatment, supplies, or medication (1) the tricare processor who sent you the form; Why does tricare send a dd form 2527? Sometimes, tricare receives claims that include diagnosis codes that may or may not relate to an injury. If a preaddressed envelope is not enclosed with this form, please return your completed form to either of these locations: Web dd form 2527, mar 2020. The beneficiary must complete and sign this form within 35 calendar days and return the. Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury.
Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. (1) the tricare processor who sent you the form; Why does tricare send a dd form 2527? The beneficiary must complete and sign this form within 35 calendar days and return the. Web dd form 2527, mar 2020. Describe condition for which patient received treatment, supplies, or medication Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury. Sometimes, tricare receives claims that include diagnosis codes that may or may not relate to an injury. Web third party liability claim form (dd2527) send third party liability form to: Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred.
Web third party liability claim form (dd2527) send third party liability form to: Why does tricare send a dd form 2527? The beneficiary must complete and sign this form within 35 calendar days and return the. If a preaddressed envelope is not enclosed with this form, please return your completed form to either of these locations: Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury. Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. Web dd form 2527, mar 2020. Sometimes, tricare receives claims that include diagnosis codes that may or may not relate to an injury. Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Describe condition for which patient received treatment, supplies, or medication
Dd Form 2527 Aug 2016 Fill Online, Printable, Fillable, Blank pdfFiller
(1) the tricare processor who sent you the form; Web dd form 2527, mar 2020. Why does tricare send a dd form 2527? Describe condition for which patient received treatment, supplies, or medication Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury.
Fillable Dd Form 2527 Statement Of Personal Injury Possible Third
Describe condition for which patient received treatment, supplies, or medication Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury. Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or.
Fillable Dd Form 2876 Tricare Prime Enrollment Application And
Web third party liability claim form (dd2527) send third party liability form to: The beneficiary must complete and sign this form within 35 calendar days and return the. Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the.
DD Form 28763 Download Fillable PDF or Fill Online TRICARE Prime
If a preaddressed envelope is not enclosed with this form, please return your completed form to either of these locations: (1) the tricare processor who sent you the form; Sometimes, tricare receives claims that include diagnosis codes that may or may not relate to an injury. Describe condition for which patient received treatment, supplies, or medication Please fill out this.

20182022 Form DD 2642 Fill Online, Printable, Fillable, Blank pdfFiller
Web dd form 2527, mar 2020. Describe condition for which patient received treatment, supplies, or medication (1) the tricare processor who sent you the form; If a preaddressed envelope is not enclosed with this form, please return your completed form to either of these locations: Web when they receive these billing statements with coding that indicates that another party may.

Dd Form 2527 Printable Printable Templates
Why does tricare send a dd form 2527? Describe condition for which patient received treatment, supplies, or medication Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. Please fill out this form to permit the.

DD Form 2876 Download Printable PDF, TRICARE Prime Enrollment
(1) the tricare processor who sent you the form; The beneficiary must complete and sign this form within 35 calendar days and return the. Web third party liability claim form (dd2527) send third party liability form to: Why does tricare send a dd form 2527? Describe condition for which patient received treatment, supplies, or medication
Fillable Dd Form 2877 Tricare Prime Disenrollment Request printable
Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Web dd form 2527, mar 2020. The beneficiary must complete and sign this form within 35 calendar days and return the. If a preaddressed envelope is not.
DD Form 3043 Download Fillable PDF or Fill Online TRICARE Select
Describe condition for which patient received treatment, supplies, or medication Sometimes, tricare receives claims that include diagnosis codes that may or may not relate to an injury. Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury. Why does tricare send a dd form 2527? Web when they receive these billing.
Dd Form 2527 ≡ Fill Out Printable PDF Forms Online
Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury. Web third party liability claim form (dd2527).
Sometimes, Tricare Receives Claims That Include Diagnosis Codes That May Or May Not Relate To An Injury.
Describe condition for which patient received treatment, supplies, or medication Why does tricare send a dd form 2527? Web third party liability claim form (dd2527) send third party liability form to: Web when tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred.
(1) The Tricare Processor Who Sent You The Form;
Web when they receive these billing statements with coding that indicates that another party may be liable for the injury, tricare management activity will send out a dd form 2527 to the tricare recipient. Web dd form 2527, mar 2020. If a preaddressed envelope is not enclosed with this form, please return your completed form to either of these locations: Please fill out this form to permit the united states to recover medical expenses from whoever caused your injury.