Express Scripts Claim Form Pdf
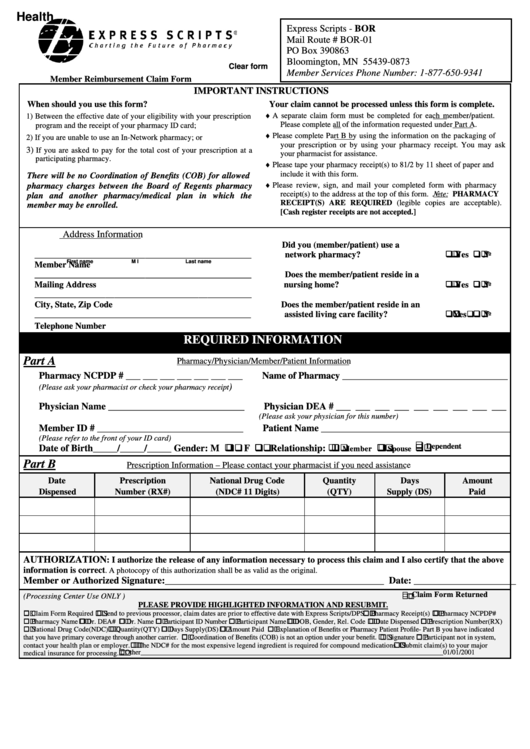
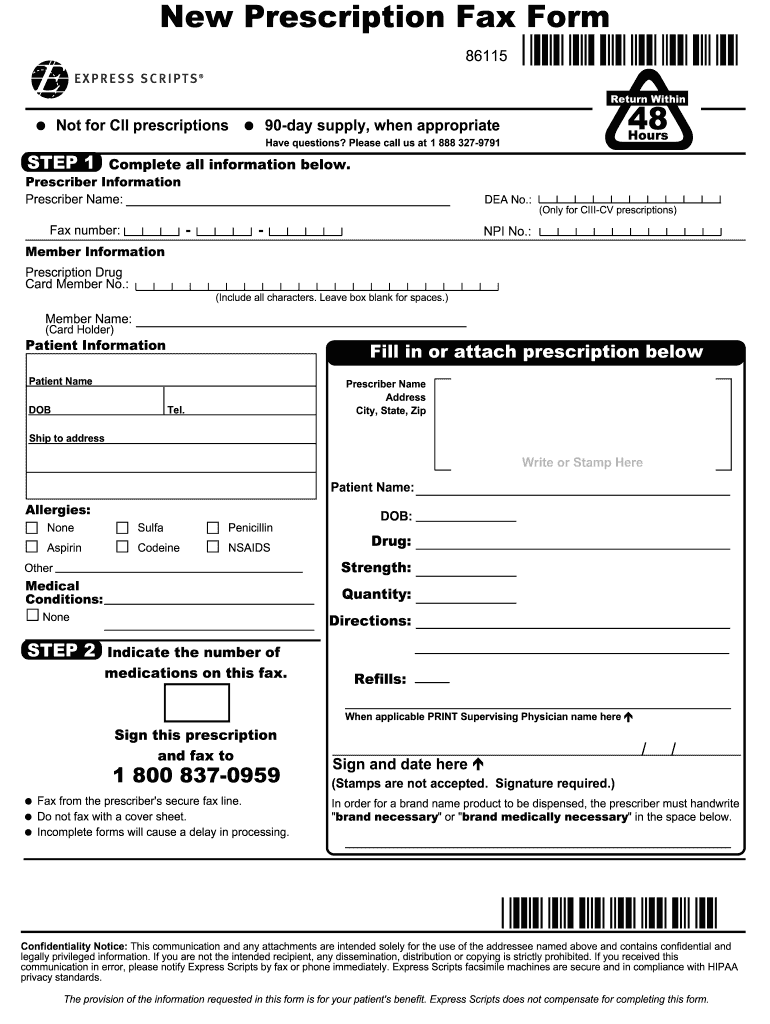
Express Scripts Claim Form Pdf - Web *if allowed by law, you may assign the payment of this claim to your pharmacy. Web send your pharmacy claims within one year of the date of service. None step 2 indicate the number of medications on this fax. Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web log in don't have an account? Print cardholder’s date of birth. Please use one claim form per. Web aspirin sulfa codeine penicillin nsaids other medical conditions: Web you can download a claim form, complete, and mail to express scripts with your receipt(s). Accessible formats are available upon request to human resources.
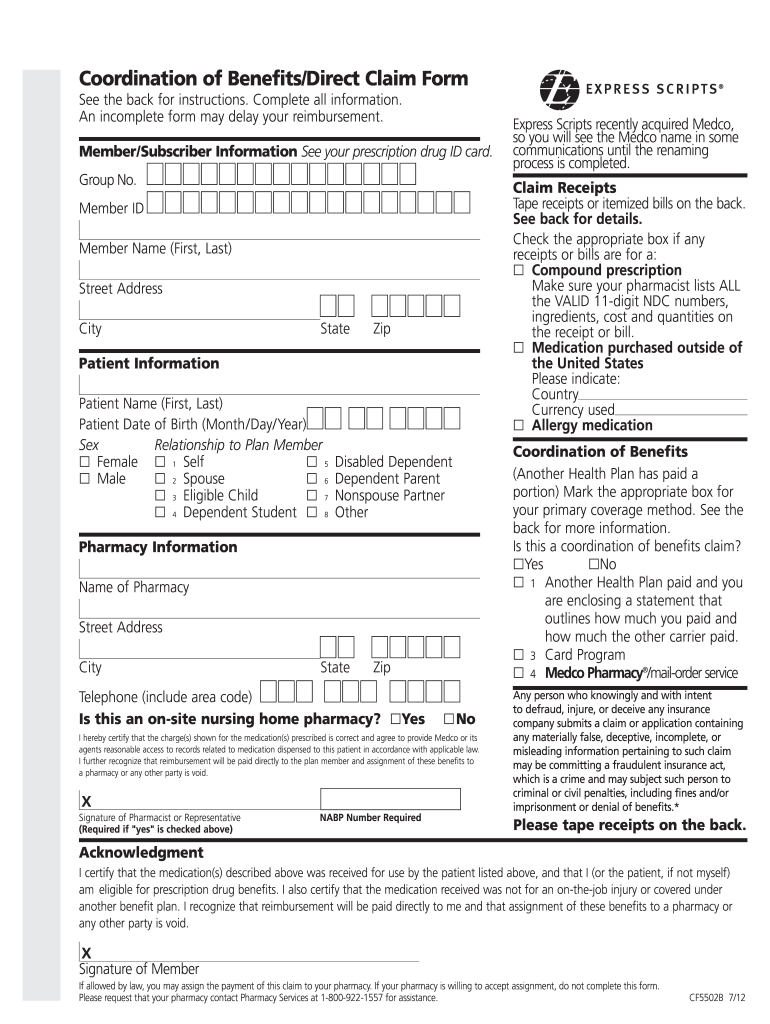
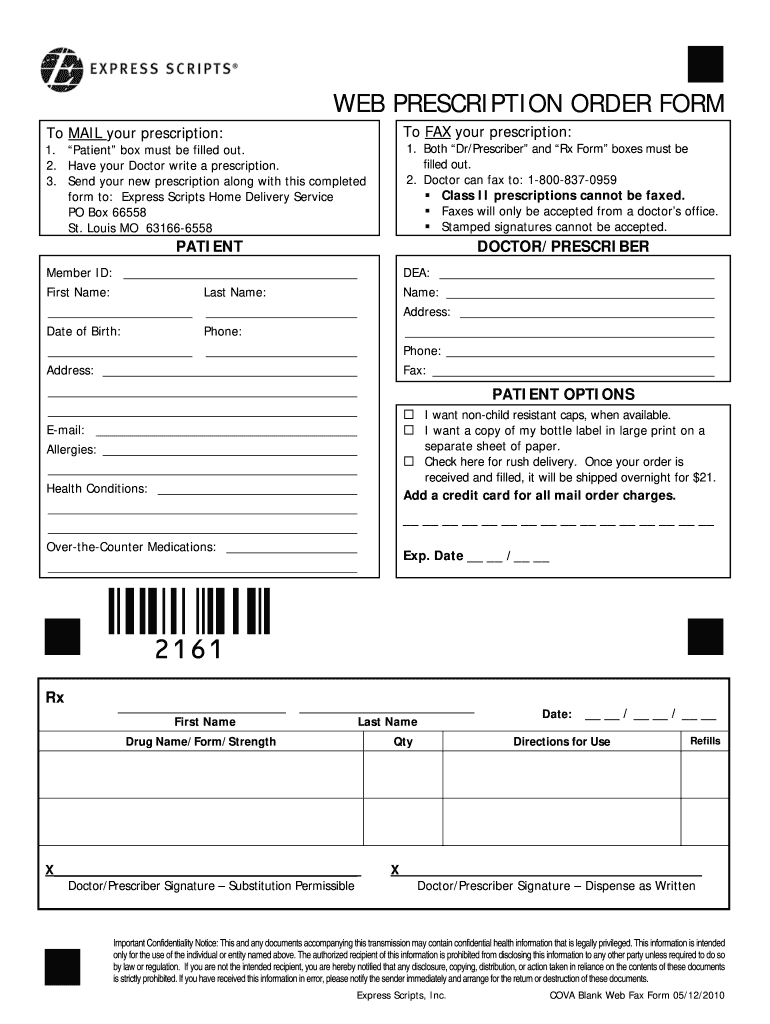
If you have other health. Web send your pharmacy claims within one year of the date of service. Web ihereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable access to records related to medic. Upload, modify or create forms. • pharmacy name/address • date filled • drug name and strength • rx. Web pharmacist resource center user guide purpose: Web the necessary information if your claim or bill is not itemized. Express scripts will process your claim(s) within 14 days of receiving all of the. Web you can download a claim form, complete, and mail to express scripts with your receipt(s). None step 2 indicate the number of medications on this fax.
Any person who knowingly and with intent. Web by signing this form, i authorize release of all information contained on this claim to express scripts, inc. The plan member should read the acknowledgment carefully, and then sign and date this form. Web aspirin sulfa codeine penicillin nsaids other medical conditions: Send the claim form and the following information for each drug. • pharmacy name/address • date filled • drug name and strength • rx. Access a comprehensive offering of the most common forms, lists and manuals. Only use this form if you are a commercial member. Web send your pharmacy claims within one year of the date of service. Web *if allowed by law, you may assign the payment of this claim to your pharmacy.
Fillable Express Scripts Claim Form printable pdf download
If your pharmacy is willing to accept assignment, do not complete this form. Web by signing this form, i authorize release of all information contained on this claim to express scripts, inc. No another health plan paid and you are enclosing a statement that outlines how much you paid and how much the other carrier. Try it for free now!.
Express Scripts Appeal Form Fill Out and Sign Printable PDF Template
Web express scripts all of the requested information for each claim to the address below. Web is this a coordination of benefits claim? Print cardholder’s name (last, first, middle initial). None step 2 indicate the number of medications on this fax. Web download the claim for reimbursement form print and complete the form mail the form and other documents to.

57 HQ Images Express Scripts Appeal Form Express Scripts Prior
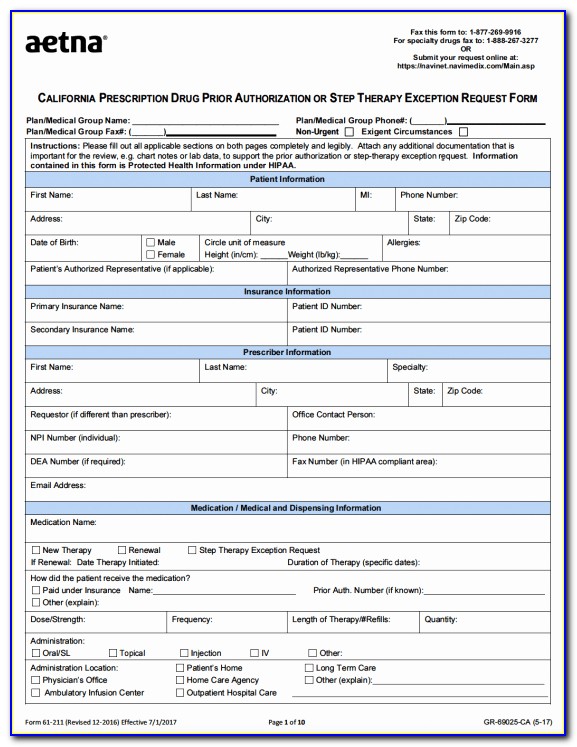
None step 2 indicate the number of medications on this fax. Web the necessary information if your claim or bill is not itemized. Only use this form if you are a commercial member. • pharmacy name/address • date filled • drug name and strength • rx. Accessible formats are available upon request to human resources.
Number of Express Scripts locations in the USA in 2023 ScrapeHero
Only use this form if you are a commercial member. Any person who knowingly and with intent. If you have other health. The plan member should read the acknowledgment carefully, and then sign and date this form. Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please download.
Express Scripts Prior Auth Form Unique Humana Prior Authorization Form
Web log in don't have an account? Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web download the claim for reimbursement form print and complete the form mail the form and other documents to the address found on the form once you submit your claim online,. Web.
Express scripts new prescription fax form Fill out & sign online DocHub
Register now we make it easy to share information get your written prescriptions to us by using our mail order form. The plan member should read the acknowledgment carefully, and then sign and date this form. The plan member should read the acknowledgment carefully, and then sign and date this form. • pharmacy name/address • date filled • drug name.
How to Get Prescription Refill Home
Express scripts will process your claim(s) within 14 days of receiving all of the. Web *if allowed by law, you may assign the payment of this claim to your pharmacy. Web aspirin sulfa codeine penicillin nsaids other medical conditions: The plan member should read the acknowledgment carefully, and then sign and date this form. Web pharmacist resource center user guide.
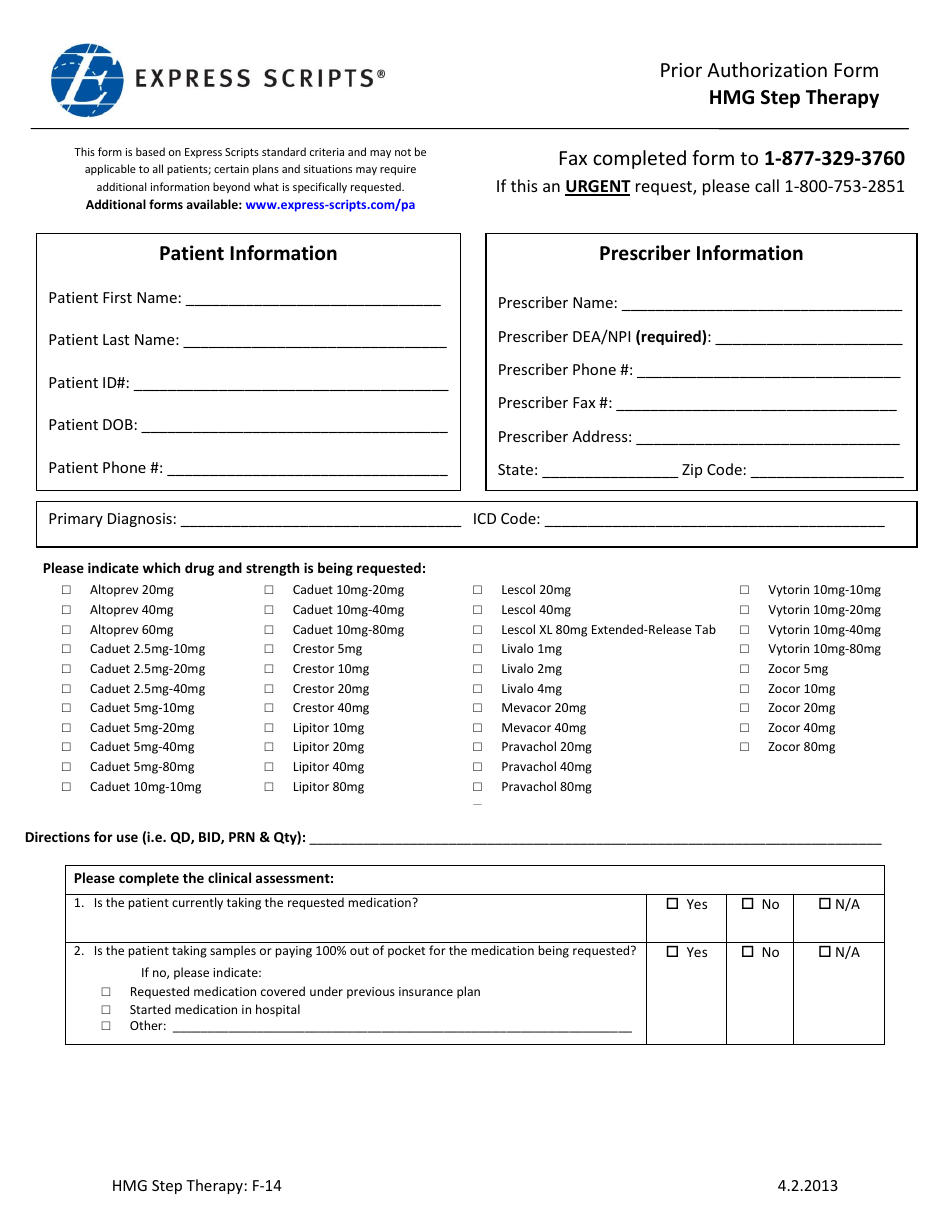
Form F14 Download Printable PDF or Fill Online Prior Authorization Form
Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Please use one claim form per. The plan member should read the acknowledgment carefully, and then sign and date this form. Web send your pharmacy claims within one year of the date of service. Web the necessary information if.
Express Scripts Fax Form Fill Online, Printable, Fillable, Blank
Circle the correct letter to indicate if cardholder is male or female. Web claims received missing any of the following information may be returned or payment may be denied. If you have other health. Web *if allowed by law, you may assign the payment of this claim to your pharmacy. Send the claim form and the following information for each.

Express Scripts Reviews Express Scripts Information Shortlister
Any person who knowingly and with intent. Web aspirin sulfa codeine penicillin nsaids other medical conditions: Try it for free now! If you have other health. Web ihereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable access to records related to medic.
Web Ihereby Certify That The Charge(S) Shown For The Medication(S) Prescribed Is Correct And Agree To Provide Express Scripts Or Its Agents Reasonable Access To Records Related To Medic.
Web you can download a claim form, complete, and mail to express scripts with your receipt(s). The plan member should read the acknowledgment carefully, and then sign and date this form. Select forms & cards (or forms) from the menu under benefit. Upload, modify or create forms.
The Plan Member Should Read The Acknowledgment Carefully, And Then Sign And Date This Form.
Web information if your claim or bill is not itemized. Accessible formats are available upon request to human resources. Web claims received missing any of the following information may be returned or payment may be denied. No another health plan paid and you are enclosing a statement that outlines how much you paid and how much the other carrier.
Web Download The Claim For Reimbursement Form Print And Complete The Form Mail The Form And Other Documents To The Address Found On The Form Once You Submit Your Claim Online,.
Web log in don't have an account? Web the necessary information if your claim or bill is not itemized. Circle the correct letter to indicate if cardholder is male or female. Web *if allowed by law, you may assign the payment of this claim to your pharmacy.
Web Aspirin Sulfa Codeine Penicillin Nsaids Other Medical Conditions:
• pharmacy name/address • date filled • drug name and strength • rx. Access a comprehensive offering of the most common forms, lists and manuals. Express scripts will process your claim(s) within 14 days of receiving all of the. Register now we make it easy to share information get your written prescriptions to us by using our mail order form.