General Health Appraisal Form
General Health Appraisal Form - Health care provider please complete if appropriate. Ad register and subscribe now to work on your piaa comprehensive initial form. None or describe type of reaction diet: Upload, modify or create forms. Please complete the following section and give to current health care provider for completion child’s name birthdate allergies: Age appropriate breast fed formula: Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Typeforms are more engaging, so you get more responses and better data. Web the colorado chapter of the american academy of pediatrics (aap) and healthy child care colorado have approved this form. Any concerns or exceptions are identified on this form.
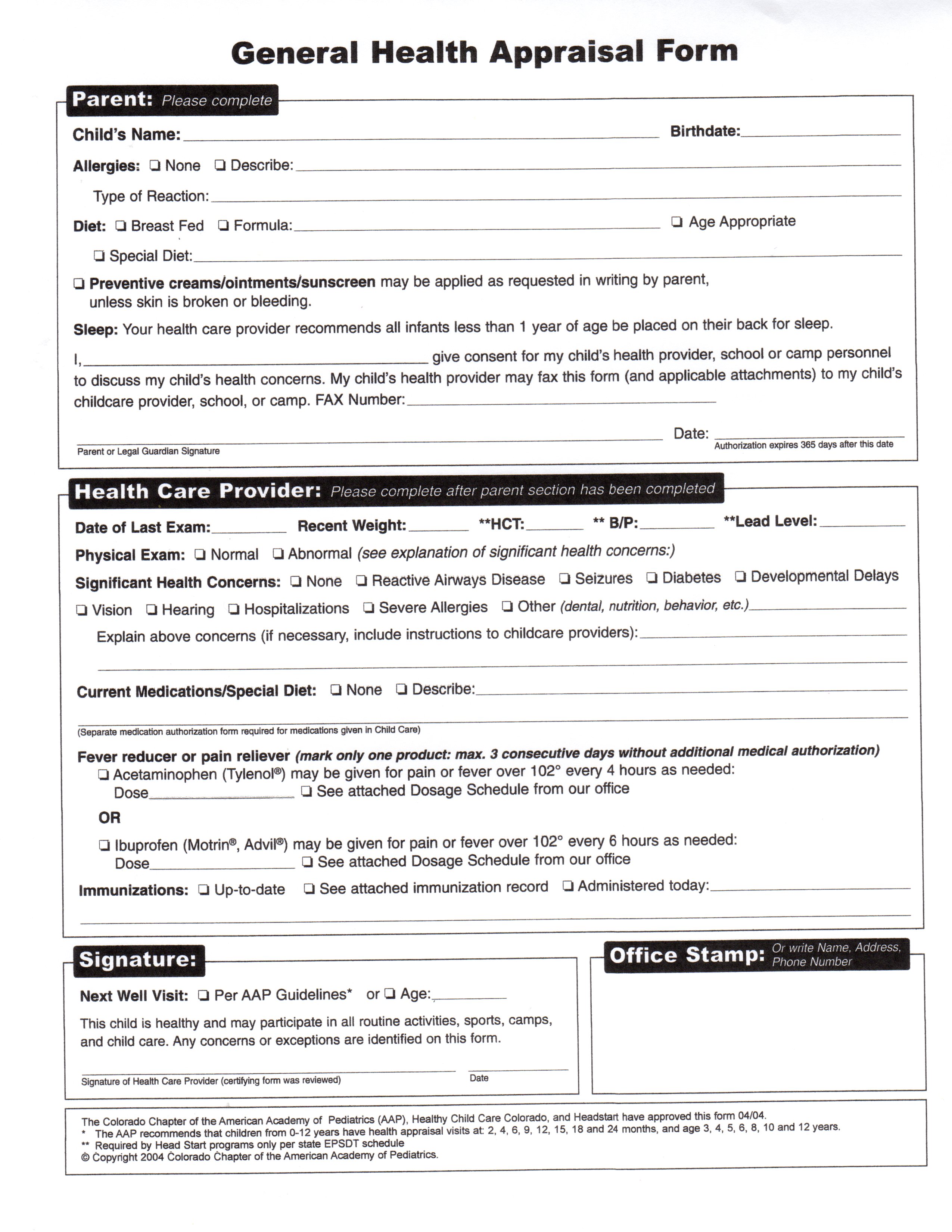
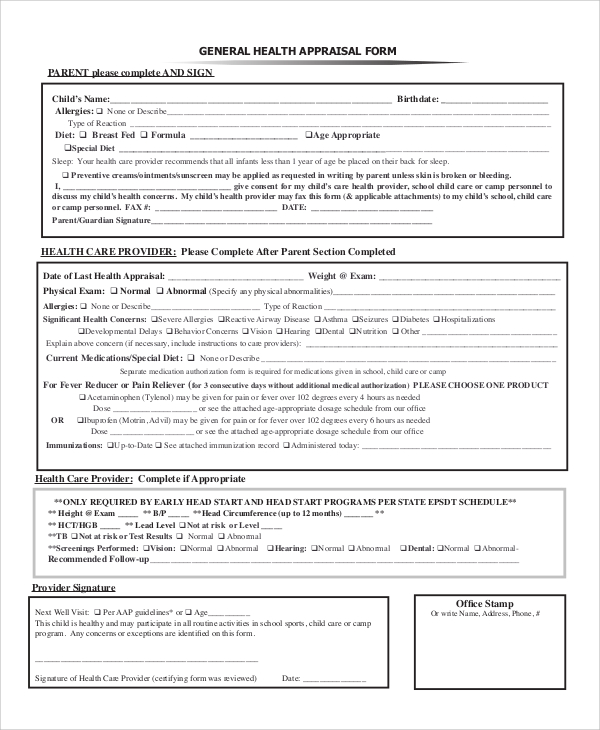
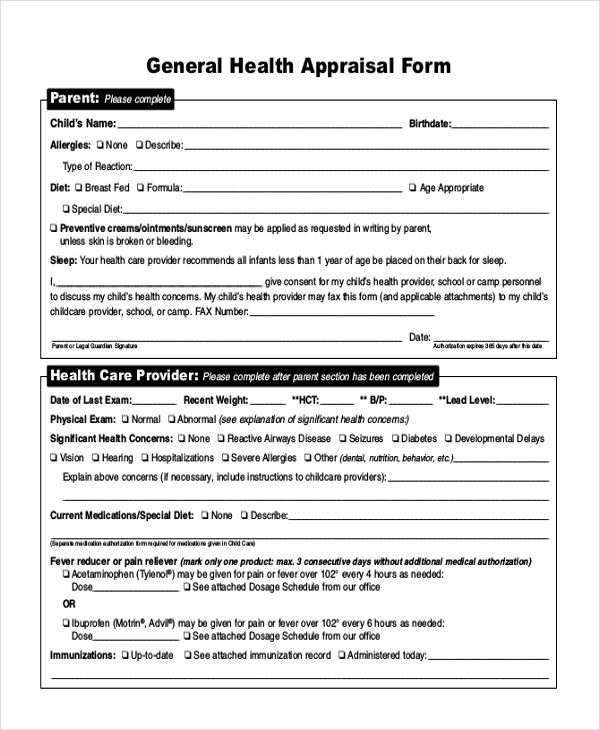
This information is required by early head start and Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Typeforms are more engaging, so you get more responses and better data. Web general health appraisal form parent please complete and sign the top portion only. None or describe type of reaction diet: Please complete the following section and give to current health care provider for completion child’s name birthdate allergies: If accurate birthdate information is included in the appraisal district records or in the information the texas department of public safety provided to the appraisal district Any concerns or exceptions are identified on this form. 2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. Health care provider please complete after parent section has been completed.
Web general health appraisal form parent please complete and sign the top portion only. Age appropriate breast fed formula: I am a resident of a facility that provides services related to health, infirmity or aging. Parent please complete, date, and sign. Breast fed formula age appropriate special diet sleep: If accurate birthdate information is included in the appraisal district records or in the information the texas department of public safety provided to the appraisal district _____ office stamp or write name, address, phone, # the colorado chapter of the american academy of pediatrics (aap) and healthy child care colorado have approved this form. _____ signature of health care provider (certifying form was reviewed) date: 2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. None or describe type of reaction diet:
General Health Appraisal Form 2015 Augustana Lutheran Church, Denver, CO
This information is required by early head start and Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Breast fed formula age appropriate special diet sleep: Or write name, address, phone number next well visit: Health care provider please complete after parent section has been completed.
FREE 6+ Sample Health Appraisal Forms in PDF
Try it for free now! Or write name, address, phone number next well visit: Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Ad register and subscribe now to work on your piaa comprehensive initial form. You can also see sales appraisal forms.
FREE 8+ Sample Health Appraisal Forms in PDF MS Word
Upload, modify or create forms. _____ signature of health care provider (certifying form was reviewed) date: None or describe type of reaction diet: Typeforms are more engaging, so you get more responses and better data. This information is required by early head start and
Medical Records Release Form Colorado gertusol88
Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Typeforms are more engaging, so you get more responses and better data. Breast fed formula age appropriate special diet sleep: You can also see sales appraisal forms. Or write name, address, phone number next well visit:
FREE 8+ Sample Health Appraisal Forms in PDF MS Word
2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. _____ signature of health care provider (certifying form was reviewed) date: Age appropriate breast fed formula: _____ office stamp or write name, address, phone, # the colorado chapter of the american academy of pediatrics (aap) and healthy child care.
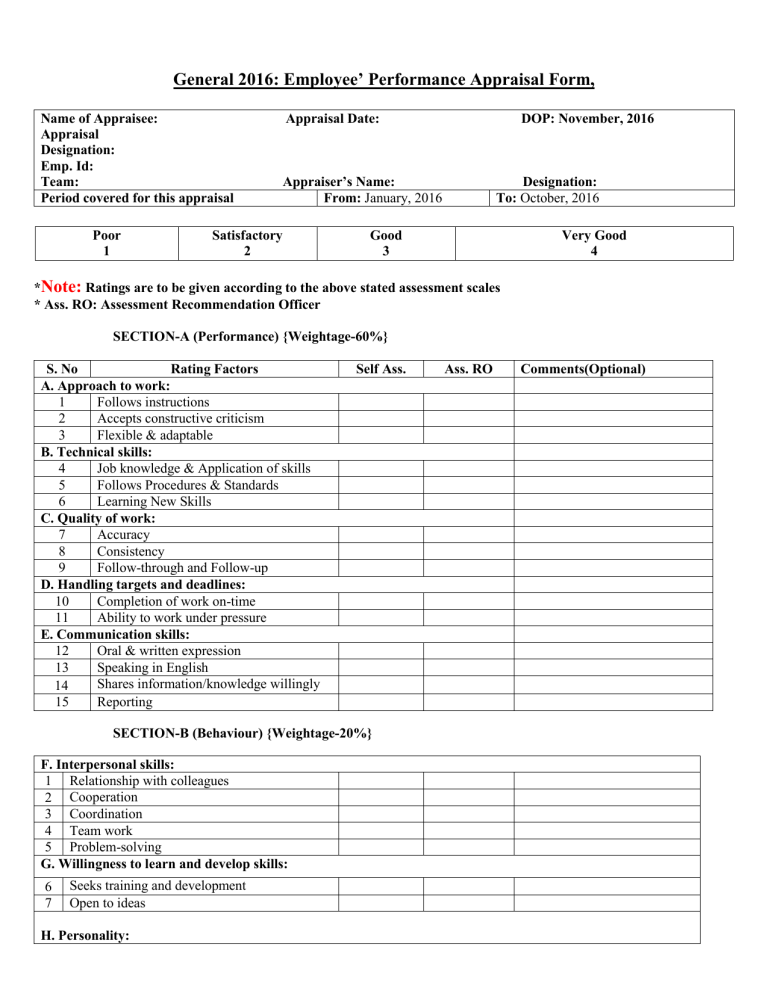
Performance Appraisal Form
Web general health appraisal form parent please complete and sign the top portion only. Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Please complete the following section and give to current health care provider for completion child’s name birthdate allergies: Health care provider please complete if appropriate. Upload,.
FREE 10+ Sample Health Appraisal Forms in PDF MS Word
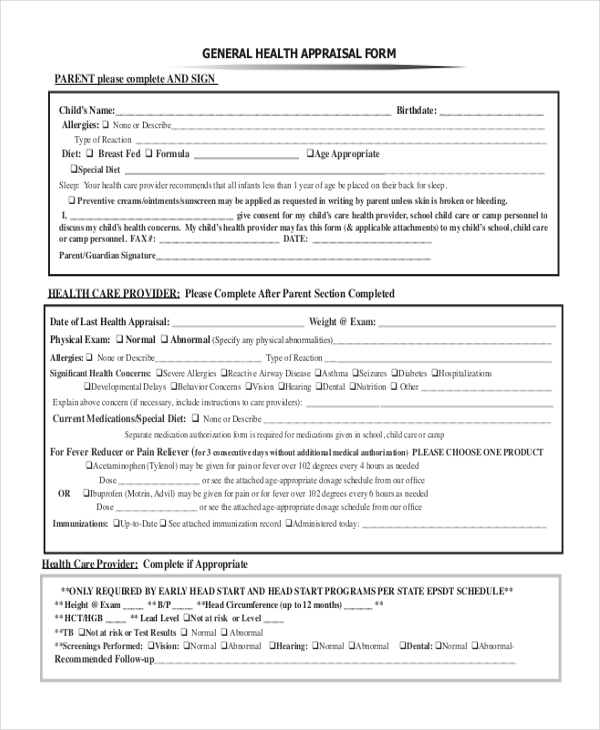
Your health care provider recommends that all infants less than 1 year of age be placed on their back for sleep. Or write name, address, phone number next well visit: Breast fed formula age appropriate special diet sleep: Web general health appraisal form parent please complete and sign the top portion only. Try it for free now!

general health appraisal form
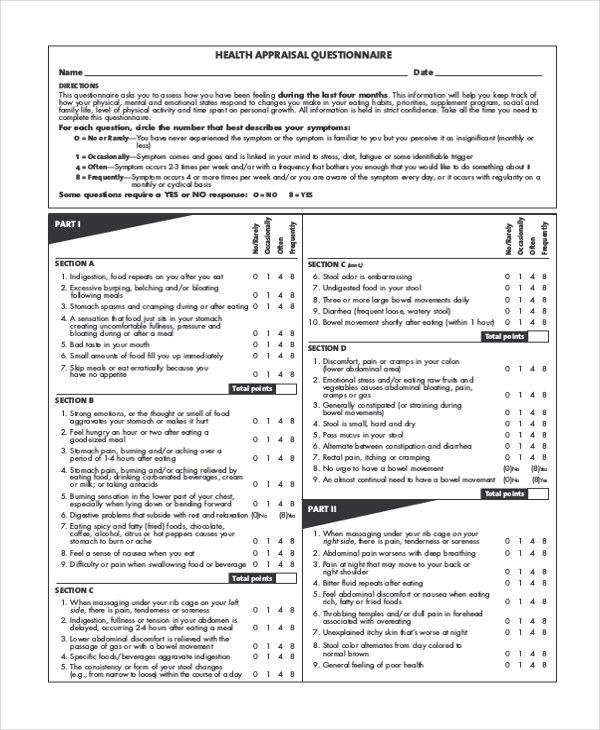
You can also see sales appraisal forms. Breast fed formula age appropriate special diet sleep: Upload, modify or create forms. Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Web this general health appraisal form is a must download for schools which wants to know about the health details.
FREE 8+ Sample Health Appraisal Forms in PDF MS Word
Web the colorado chapter of the american academy of pediatrics (aap) and healthy child care colorado have approved this form. You can also see sales appraisal forms. Web general health appraisal form parent please complete and sign the top portion only. This information is required by early head start and Health care provider please complete if appropriate.
General health appraisal form
Your health care provider recommends that all infants less than 1 year of age be placed on their back for sleep. None or describe type of reaction diet: 2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. I am a resident of a facility that provides services related.
Web General Health Appraisal Form Parent Please Complete And Sign The Top Portion Only.
2, 4, 6, 9, 12, 15, 18 and 24 months, and age 3, 4, 5, 6, 8, 10 and 12 years. I am a resident of a facility that provides services related to health, infirmity or aging. Per aap guidelines* or age:_____________________________ this child is healthy and may participate in all routine activities, sports, camps,and child care. Your health care provider recommends that all infants less than 1 year of age be placed on their back for sleep.
Typeforms Are More Engaging, So You Get More Responses And Better Data.
_____ office stamp or write name, address, phone, # the colorado chapter of the american academy of pediatrics (aap) and healthy child care colorado have approved this form. If accurate birthdate information is included in the appraisal district records or in the information the texas department of public safety provided to the appraisal district This information is required by early head start and None or describe type of reaction diet:
Please Complete The Following Section And Give To Current Health Care Provider For Completion Child’s Name Birthdate Allergies:
_____ signature of health care provider (certifying form was reviewed) date: Health care provider please complete if appropriate. Try it for free now! Web the colorado chapter of the american academy of pediatrics (aap) and healthy child care colorado have approved this form.
Breast Fed Formula Age Appropriate Special Diet Sleep:
Upload, modify or create forms. Health care provider please complete after parent section has been completed. You can also see sales appraisal forms. Age appropriate breast fed formula: