Humana Grievance And Appeal Form
Humana Grievance And Appeal Form - Commercial health benefits claims form commercial pharmacy claims form. You may be able to appeal humana’s decision if your medication is not approved. Web if you believe that humana inc. You can use this form to tell us what. We will get some information from you and start the appeal process. Please submit the appeal online via availity. Legal representatives for humana members may request a grievance or appeal on behalf of a humana member. Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. Web appeals:all appeals for claim denial1(or any decision that does not cover expenses you believe should have been covered) must be sent to grievance and appeals you may. Web grievance/appeal request form you may complete the form with information about the member whose treatment is the subject of the grievance/appeal.
You may be able to appeal humana’s decision if your medication is not approved. Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. To file an appeal, please download and complete the. Web humana grievance and appeal department appointment of authorized representative form. Member name member id number (to be completed by. Web appeals:all appeals for claim denial1(or any decision that does not cover expenses you believe should have been covered) must be sent to grievance and appeals you may. Fax or mail the form. Web humana grievance and appeal department appointment of authorized representative form. Please submit the appeal online via availity. Grievance and appeal department p.o.
Web humana grievance and appeal department appointment of authorized representative form. Web if you believe that humana inc. Web 1 comments 0 followers find out most commonly used forms via our humana website below: Or its subsidiaries have failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability,. Download a copy of the following form and fax or mail it to humana: Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. We will get some information from you and start the appeal process. Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. Fax or mail the form. Web submit an appeal or grievance for a loved one.

Humana Prior Authorization form Medication Lovely Drug Channels
Web 1 comments 0 followers find out most commonly used forms via our humana website below: Web if you don’t agree with humana’s decision. Grievance and appeal department p.o. Web submit an appeal or grievance for a loved one. Fax or mail the form.

Humana Pharmacy Physician Fax form Brilliant Humana Appeal form
Or its subsidiaries have failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability,. Web if filing on your own behalf, you need to submit your written request within the time frame established by applicable state law. Web humana grievance and appeal department appointment of authorized representative form. Web humana.
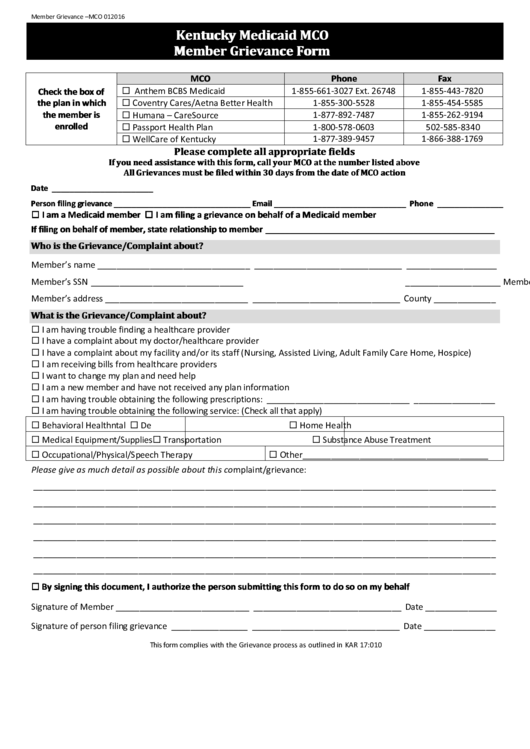
Fillable Kentucky Medicaid Mco Member Grievance Form printable pdf download
Download a copy of the following form and fax or mail it to humana: Member name member id number (to be completed by. Grievance and appeal department p.o. Commercial health benefits claims form commercial pharmacy claims form. You may be able to appeal humana’s decision if your medication is not approved.
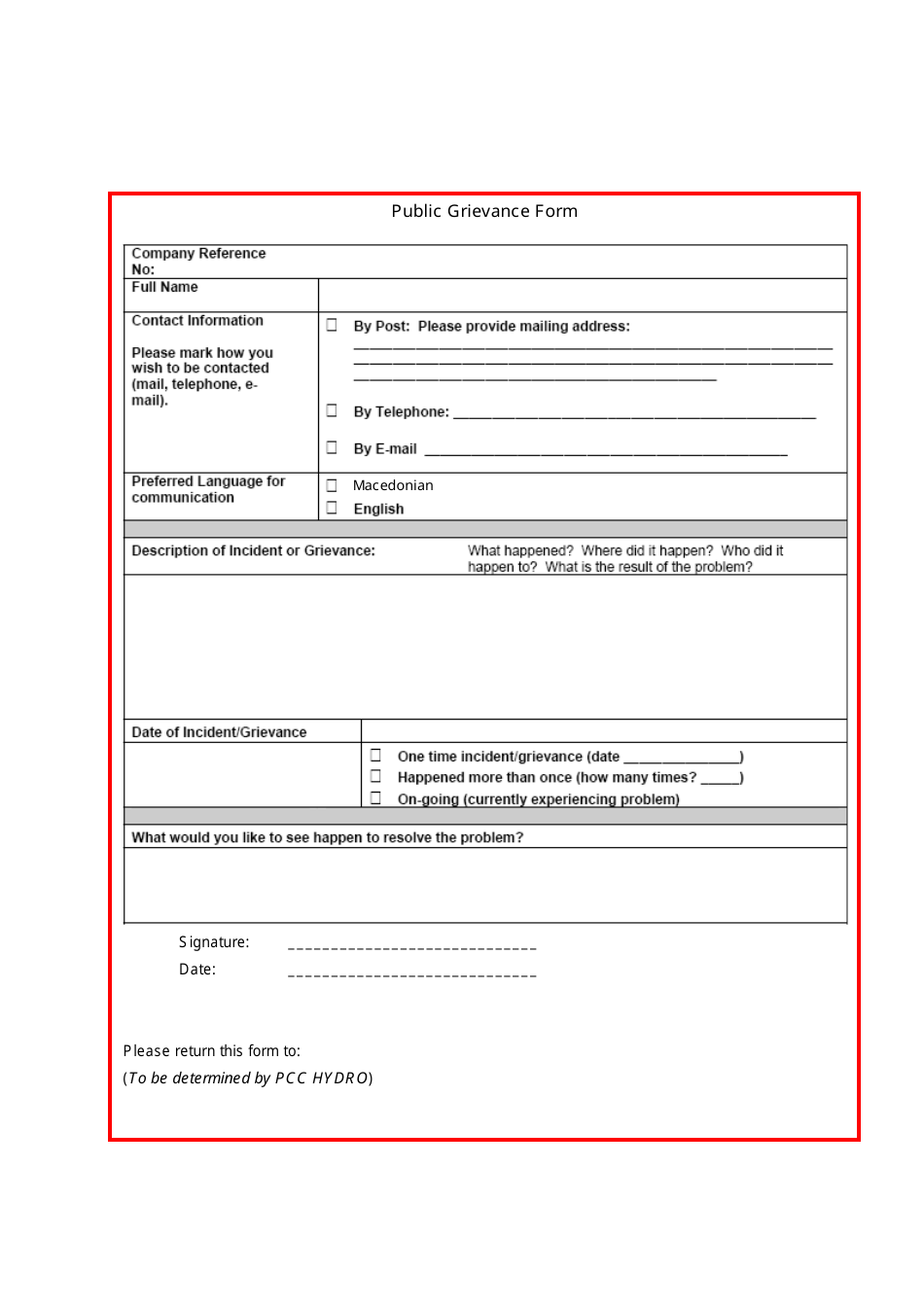
Public Grievance Form Download Printable PDF Templateroller
Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. Fax or mail the form. Or its subsidiaries have failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability,. Web if filing on your own behalf, you need to.

FREE 9+ Member Complaint Forms in PDF Ms Word
Legal representatives for humana members may request a grievance or appeal on behalf of a humana member. Web if you don’t agree with humana’s decision. Fax or mail the form. Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. We will get some information from you and start.
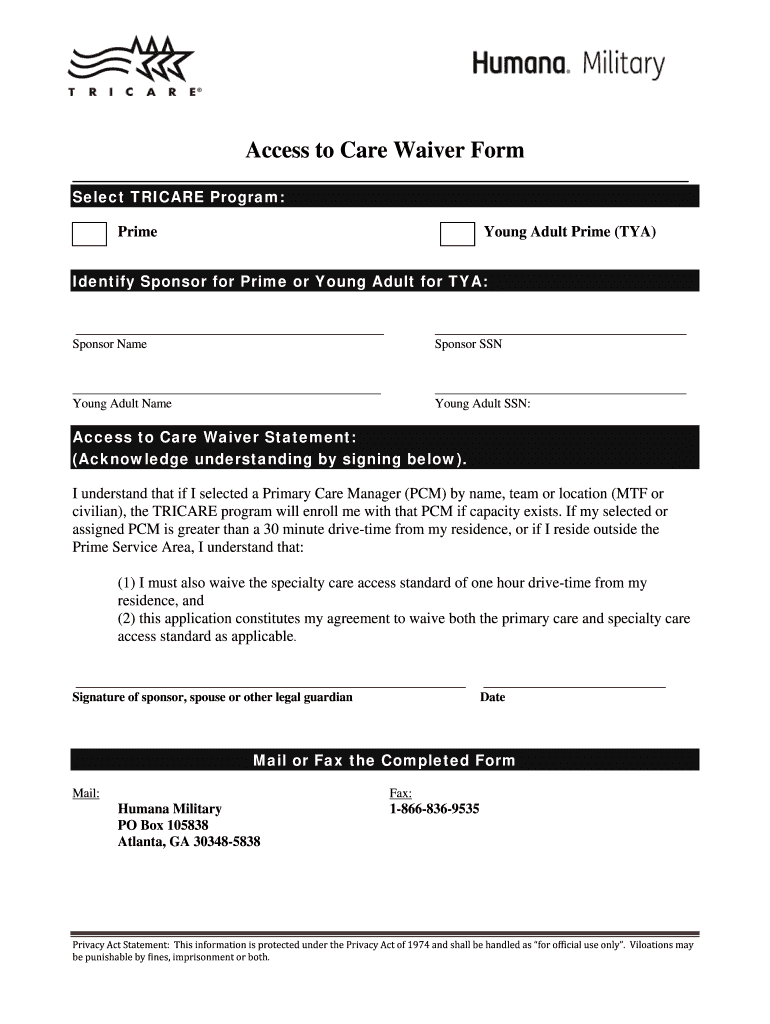
Humana Military Access to Care Waiver Form Fill and Sign Printable
Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. Legal representatives for humana members may request a grievance or.

How to File a Grievance or Appeal Related to Your Kentucky Medicaid
Web grievance/appeal request form you may complete the form with information about the member whose treatment is the subject of the grievance/appeal. Web humana grievance and appeal department appointment of authorized representative form. Web submit an appeal or grievance for a loved one. You can use this form to tell us what. Web if you don’t agree with humana’s decision.
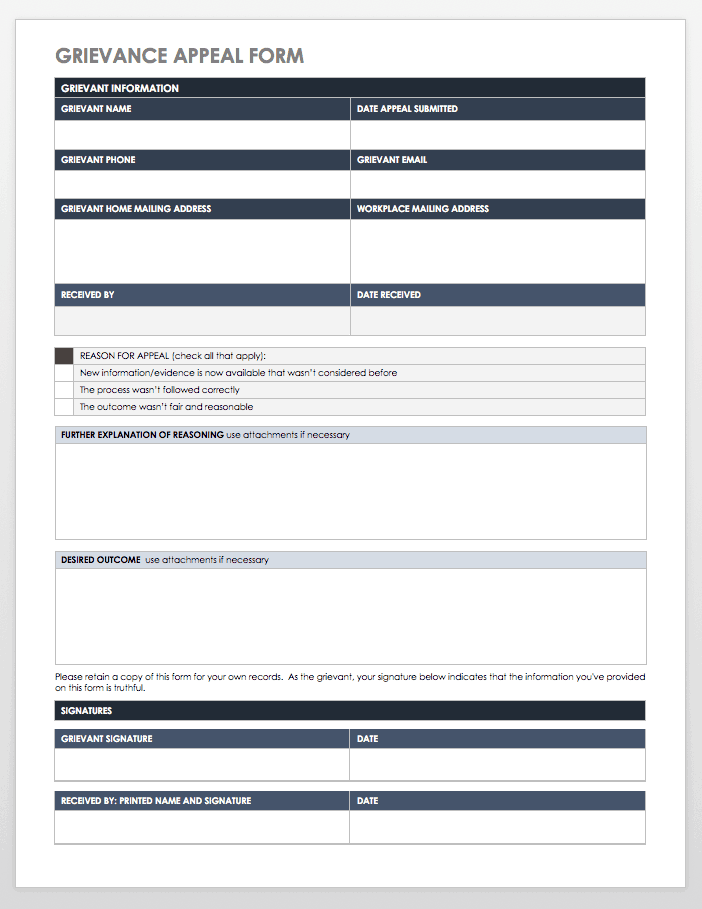
Free Grievance Form Templates Smartsheet
Commercial health benefits claims form commercial pharmacy claims form. Grievance and appeal department p.o. Please submit the appeal online via availity. Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. Web grievance/appeal request form please complete this form with information.

Humana Insurance Claim Form Financial Report
Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. Download a copy of the following form and fax or mail it to humana: Filing a grievance or appeal online use. We will get some information from you and start the.
Step 2 grievance appeal form apwulocal197
Web online request for appeals, complaints and grievances. Filing a grievance or appeal online use. You can use this form to tell us what. We will get some information from you and start the appeal process. Web if you don’t agree with humana’s decision.
Member Name Member Id Number (To Be Completed By.
Web grievance or appeal form if you have a grievance or appeal related to your careplus plan or any aspect of your care, we want to hear about it. Or its subsidiaries have failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability,. Legal representatives for humana members may request a grievance or appeal on behalf of a humana member. Web submit an appeal or grievance for a loved one.
You Can Use This Form To Tell Us What.
Web appeal, complaint or grievance form if you have a complaint or appeal related to your humana plan or any aspect of your care, we want to hear about it and see how we can. Web grievance/appeal request form please complete this form with information about the member whose treatment is the subject of the grievance/appeal. Web online request for appeals, complaints and grievances. We will get some information from you and start the appeal process.
Web If Filing On Your Own Behalf, You Need To Submit Your Written Request Within The Time Frame Established By Applicable State Law.
Grievance and appeal department p.o. Web if you believe that humana inc. Download a copy of the following form and fax or mail it to humana: Please submit the appeal online via availity.
Web Grievance/Appeal Request Form You May Complete The Form With Information About The Member Whose Treatment Is The Subject Of The Grievance/Appeal.
Web 1 comments 0 followers find out most commonly used forms via our humana website below: To file an appeal, please download and complete the. Web humana grievance and appeal department appointment of authorized representative form. Fax or mail the form.