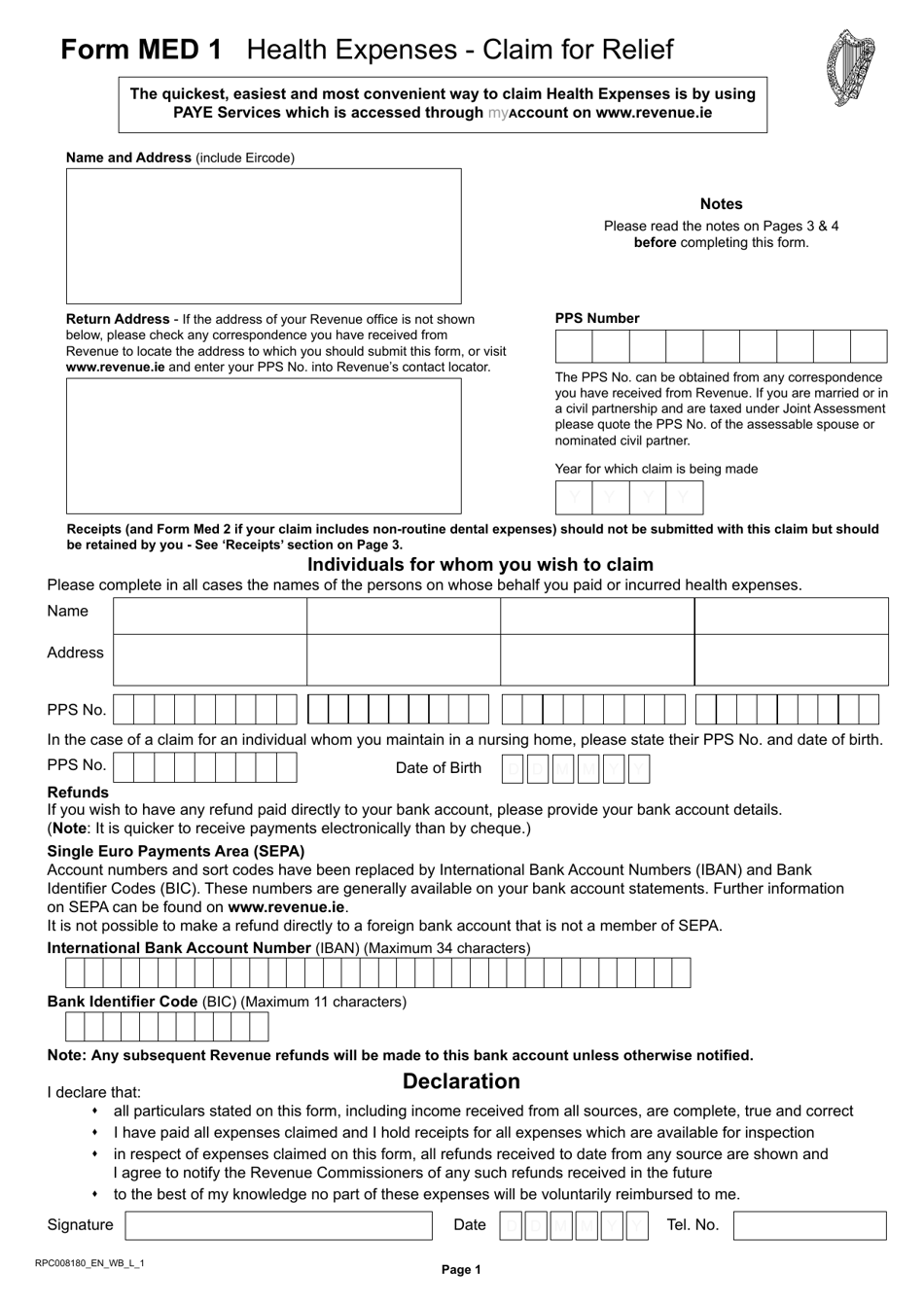
Med 1 Form
Med 1 Form - Download location map and hours. A copy of the form is attached in the appendix to these materials. Examination report wfnj case number: Web form med 1 (r 2009) section d: Social security number date of birth: Please do not return the completed form to the client. The information given by me on this form is true and correct to the best of my knowledge and belief. If they have been approved for temporary disability benefits and wish to extend their claim further, they will provide you with printed. Easily fill out pdf blank, edit, and sign them. Claimant’ s declaration (to be completed by the claimant) i declare that:
Claimant’ s declaration (to be completed by the claimant) i declare that: Easily fill out pdf blank, edit, and sign them. If they have been approved for temporary disability benefits and wish to extend their claim further, they will provide you with printed. I am incapable of work and have done no paid work since the date shown at question 38. Web how you can complete the won med 1 form on the internet: Web form med 1 (r 2009) section d: Code 61602445400 distribution of copies: Your patient has requested that medication. Please do not return the completed form to the client. The information given by me on this form is true and correct to the best of my knowledge and belief.
Your patient has requested that medication. Web please send the completed form directly to the office indicated below. Easily fill out pdf blank, edit, and sign them. Examination report wfnj case number: To get started on the document, utilize the fill camp; Web provide employees with information on where to go, what to expect, and what to do. Web how you can complete the won med 1 form on the internet: Claimant’ s declaration (to be completed by the claimant) i declare that: 12/13) state of north carolina north carolina department of transportation division of motor vehicles medical certification of driver type for commercial driver license name (first) ( middle) (last ) (suffix) north carolina license number: I am incapable of work and have done no paid work since the date shown at question 38.
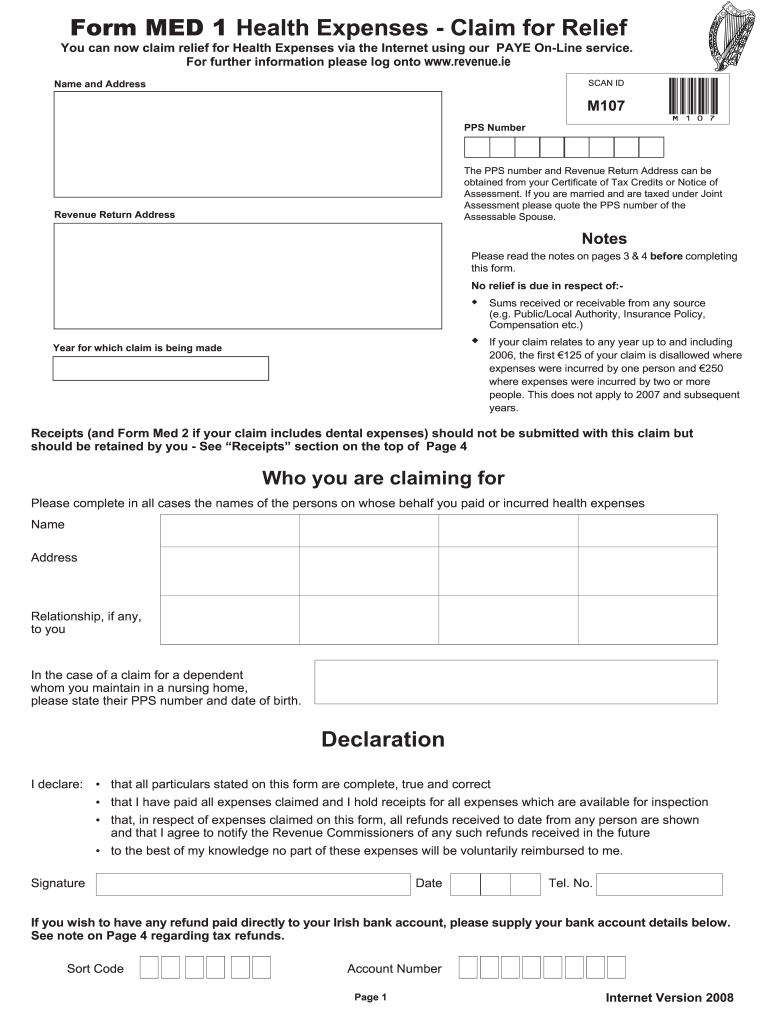
Form MED1 Download Fillable PDF or Fill Online Health Expenses Claim
Download location map and hours. Please do not return the completed form to the client. The information given by me on this form is true and correct to the best of my knowledge and belief. My last day at work was _____. Document the process for future verification and hipaa requirements.

Med 1 Form Fill Online, Printable, Fillable, Blank pdfFiller
12/13) state of north carolina north carolina department of transportation division of motor vehicles medical certification of driver type for commercial driver license name (first) ( middle) (last ) (suffix) north carolina license number: Web submit a medical certification. Web form med 1 (r 2009) section d: Enter your official identification and contact details. Easily fill out pdf blank, edit,.

Share on Twitter Facebook Google
Please do not return the completed form to the client. Web please send the completed form directly to the office indicated below. Your patient has requested that medication. Web submit a medical certification. To get started on the document, utilize the fill camp;
Med 1 Form Fill Online, Printable, Fillable, Blank pdfFiller
Code 61602445400 distribution of copies: Your patient has requested that medication. Social security number date of birth: If they have been approved for temporary disability benefits and wish to extend their claim further, they will provide you with printed. Web provide employees with information on where to go, what to expect, and what to do.

VA MED 4 20162021 Fill and Sign Printable Template Online US Legal
Social security number date of birth: Your patient has requested that medication. Sign online button or tick the preview image of the blank. Save or instantly send your ready documents. Web submit a medical certification.

10+ Medical Certificate Samples MS Word, Excel & PDF Formats, Samples
To get started on the document, utilize the fill camp; Easily fill out pdf blank, edit, and sign them. Document the process for future verification and hipaa requirements. Web provide employees with information on where to go, what to expect, and what to do. The information given by me on this form is true and correct to the best of.

Med One form Nj Awesome Two Separate Signals Act Independently to
Web how you can complete the won med 1 form on the internet: Enter your official identification and contact details. The information given by me on this form is true and correct to the best of my knowledge and belief. Web please send the completed form directly to the office indicated below. Code 61602445400 distribution of copies:

New Jersey Medical Release Form 1 PDFSimpli
If they have been approved for temporary disability benefits and wish to extend their claim further, they will provide you with printed. Examination report wfnj case number: Download location map and hours. My last day at work was _____. Document the process for future verification and hipaa requirements.
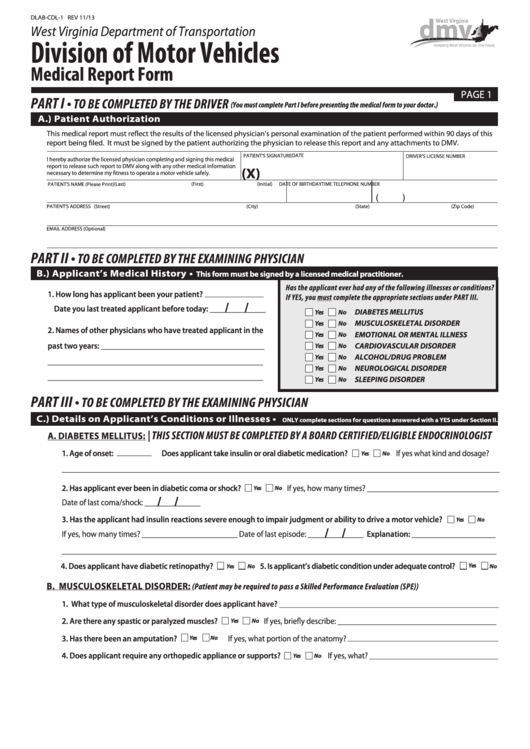
Form DlabCdl1 Medical Report Form printable pdf download
Web how you can complete the won med 1 form on the internet: Sign online button or tick the preview image of the blank. A copy of the form is attached in the appendix to these materials. Web form med 1 (r 2009) section d: Code 61602445400 distribution of copies:

1+ New Jersey Certified Payroll Form Free Download
Enter your official identification and contact details. If they have been approved for temporary disability benefits and wish to extend their claim further, they will provide you with printed. A copy of the form is attached in the appendix to these materials. Web submit a medical certification. Web please send the completed form directly to the office indicated below.
Web How You Can Complete The Won Med 1 Form On The Internet:
Claimant’ s declaration (to be completed by the claimant) i declare that: Web form med 1 (r 2009) section d: The advanced tools of the editor will lead you through the editable pdf template. My last day at work was _____.
Social Security Number Date Of Birth:
I am incapable of work and have done no paid work since the date shown at question 38. Download location map and hours. Your patient has requested that medication. Please do not return the completed form to the client.
If They Have Been Approved For Temporary Disability Benefits And Wish To Extend Their Claim Further, They Will Provide You With Printed.
12/13) state of north carolina north carolina department of transportation division of motor vehicles medical certification of driver type for commercial driver license name (first) ( middle) (last ) (suffix) north carolina license number: The information given by me on this form is true and correct to the best of my knowledge and belief. Sign online button or tick the preview image of the blank. Enter your official identification and contact details.
Web Please Send The Completed Form Directly To The Office Indicated Below.
Save or instantly send your ready documents. Web submit a medical certification. To get started on the document, utilize the fill camp; Examination report wfnj case number: