Medical Clearance Form For Dental Treatment
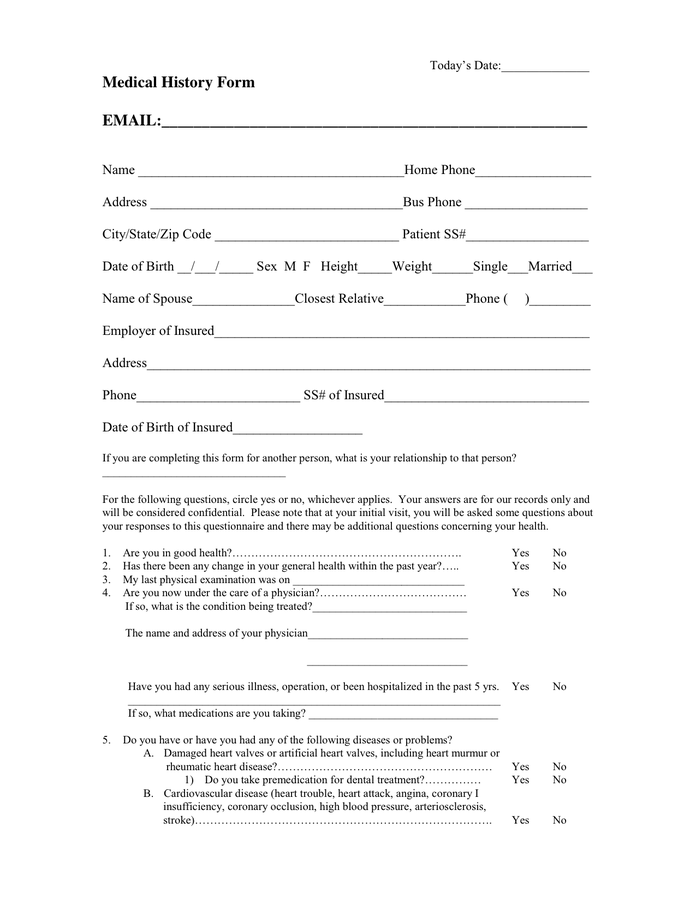
Medical Clearance Form For Dental Treatment - Fill & download for free get form download the form the guide of drawing up medical clearance form for dental online if you take an interest in customize and create a medical clearance form for dental, here are the easy guide you need to follow: Hit the get form button on this page. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web medical clearance for dental treatment date: _____ dear dental provider, our mutual patient is in need of dental treatment. Web medical clearance for dental treatment date:___________________________ attention:________________________ patient:________________________ dear dr. Web we appreciate your assistance in providing optimum care for our patient. Our mutual patient, as noted above, is scheduled for dental treatment at our office. The form is available in a digital, downloadable version or in print. Cleaning (simple or deep) radiographs with appropriate abdominal shielding
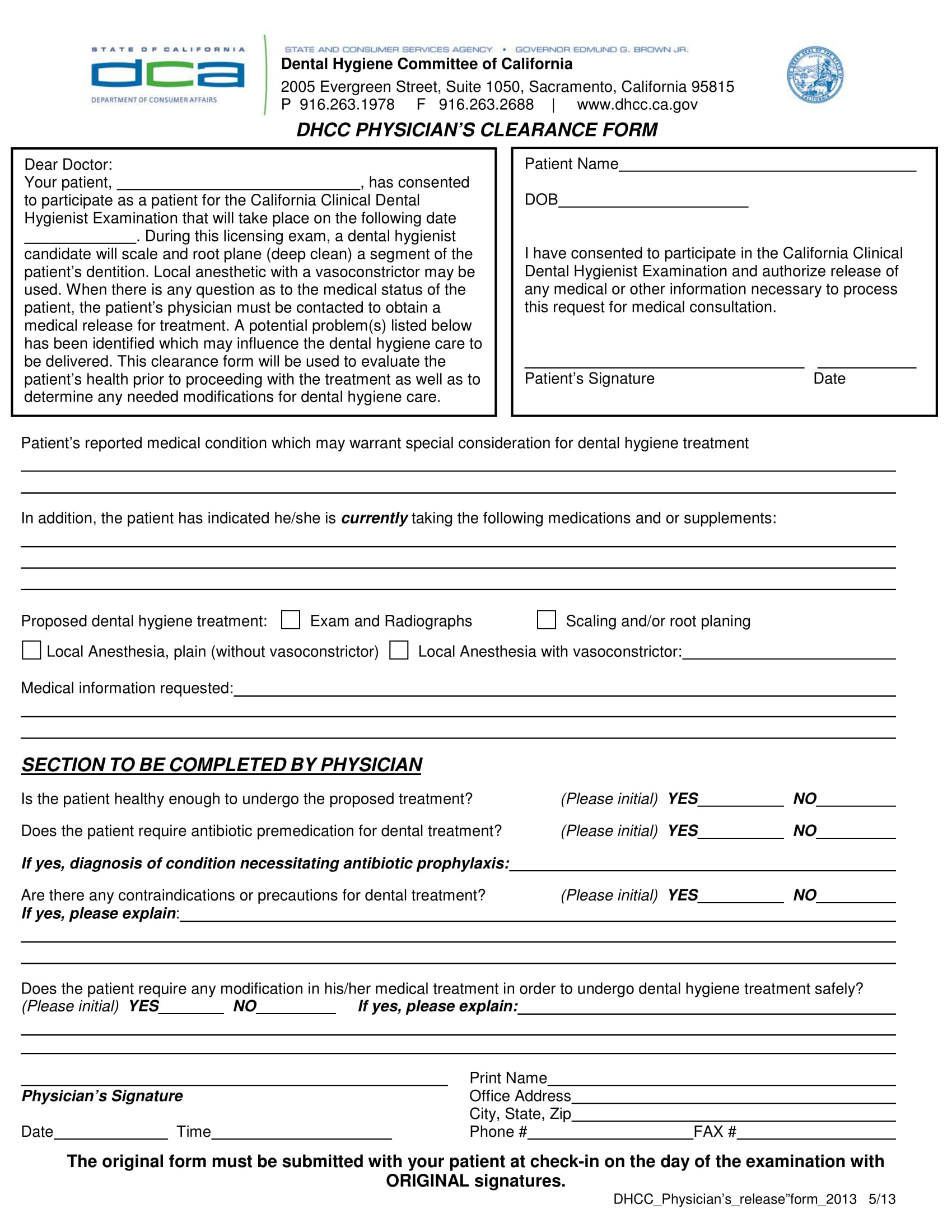
Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Web we appreciate your assistance in providing optimum care for our patient. Web medical clearance form for dental: Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Hit the get form button on this page. Cleaning (simple or deep) radiographs with appropriate abdominal shielding Web medical clearance for dental treatment date: Our mutual patient, as noted above, is scheduled for dental treatment at our office. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Please complete this form entirely so that we can safely render the best possible dental care for our mutual patient.
Treatment may include (any exclusions will be lined through): Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web medical clearance for dental treatment date:___________________________ attention:________________________ patient:________________________ dear dr. _________________________ dob:____________ our mutual patient, ________________________ ________ is scheduled for dental treatment. Web dental medical clearance forms are documents which are provided by an individual’s dentist and addressed to the physician who will administer a set of medical examinations to the individual or the dentist’ patient. Web we appreciate your assistance in providing optimum care for our patient. Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: 31st street suite a, temple, tx 76504 • phone: Web medical clearance for dental treatment date: Cleaning (simple or deep) radiographs with appropriate abdominal shielding
Physician Clearance For Dental Treatment Form printable pdf download
Treatment may include (any exclusions will be lined through): Our mutual patient, as noted above, is scheduled for dental treatment at our office. Cleaning (simple or deep) radiographs with appropriate abdominal shielding _____ dear dental provider, our mutual patient is in need of dental treatment. Web this article presents recommendations related to patients with certain medical conditions who are planning.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web we appreciate your assistance in providing optimum care for our patient. Please sign and fax form to: Web medical clearance for dental treatment date:___________________________ attention:________________________ patient:________________________ dear dr. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease, abscessed teeth, fractured teeth or fillings, loose teeth or other oral pathology and no anticipation of dental care within the next 6 months. Web dental medical clearance forms.
FREE 30+ Medical Clearance Form Samples in PDF MS Word
Web medical clearance for dental treatment date: Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease, abscessed teeth, fractured teeth or fillings, loose teeth or other oral pathology and no anticipation of dental care within the next.
FREE 31+ Medical Clearance Forms in PDF MS Word
Hit the get form button on this page. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease, abscessed teeth, fractured teeth or fillings, loose teeth or other oral pathology and no anticipation of dental care within the.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. _________________________ dob:____________ our mutual patient, ________________________ ________ is scheduled for dental treatment. The form is available in a digital, downloadable version or in print. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of.
FREE 30+ Medical Clearance Form Samples in PDF MS Word
The form is available in a digital, downloadable version or in print. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. _____ dear dental provider, our mutual patient is in need of dental treatment. 31st street suite a, temple, tx 76504.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Our mutual patient, as noted above, is scheduled for dental treatment at our office. Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: Web medical clearance for dental treatment date:___________________________ attention:________________________ patient:________________________ dear dr. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Web prior to surgery, it is.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web dental medical clearance forms are documents which are provided by an individual’s dentist and addressed to the physician who will administer a set of medical examinations to the individual or the dentist’ patient. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental.
Medical Clearance Form For Dental Treatment templates free printable
_____ dear dental provider, our mutual patient is in need of dental treatment. 31st street suite a, temple, tx 76504 • phone: Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Web medical clearance for dental treatment date: Please complete this form entirely so that we can safely render the best possible dental.
Web Medical Clearance For Dental Treatment Date:
Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease, abscessed teeth, fractured teeth or fillings, loose teeth or other oral pathology and no anticipation of dental care within the next 6 months. 31st street suite a, temple, tx 76504 • phone: Our mutual patient, as noted above, is scheduled for dental treatment at our office. Web medical clearance form for dental:
Web Medical Clearance For Dental Treatment Patient’s Name:_________________________ D.o.b:______________ Date Of Last Physical Exam:_____________ Dear Physician:
Cleaning (simple or deep) radiographs with appropriate abdominal shielding Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: Web medical clearance for dental treatment date:___________________________ attention:________________________ patient:________________________ dear dr. Fill & download for free get form download the form the guide of drawing up medical clearance form for dental online if you take an interest in customize and create a medical clearance form for dental, here are the easy guide you need to follow:
Hit The Get Form Button On This Page.
Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web we appreciate your assistance in providing optimum care for our patient. The form is available in a digital, downloadable version or in print.
Web Medical Clearance For Dental Treatment Date:
Treatment may include (any exclusions will be lined through): Please sign and fax form to: _________________________ dob:____________ our mutual patient, ________________________ ________ is scheduled for dental treatment. _____ dear dental provider, our mutual patient is in need of dental treatment.