Medicare Form Cms1490S
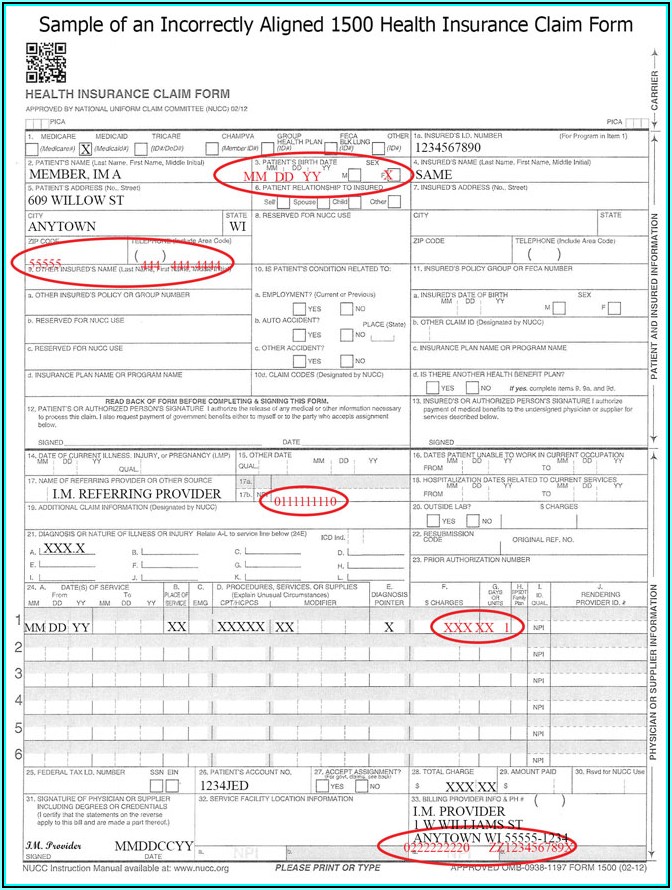
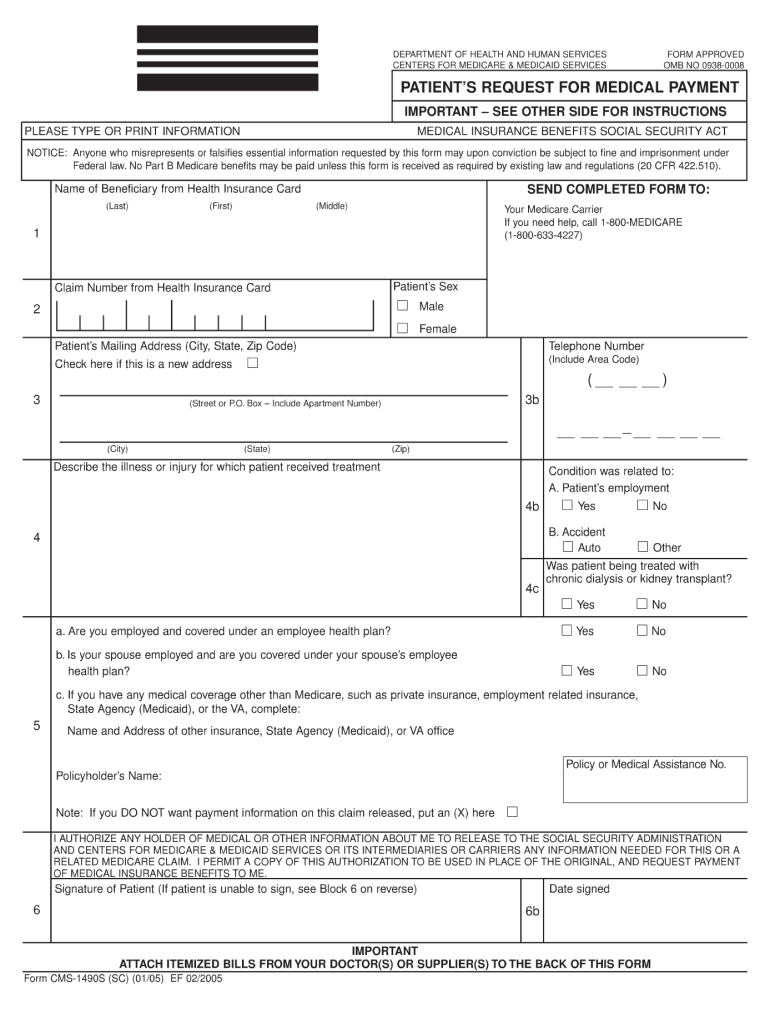
Medicare Form Cms1490S - Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web (first) (middle) claim number from health insurance card send completed form to: This particular form is known as the patient’s request for medical payment form. Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services), durable medical. Your bill does not have to be paid before you submitthis claim for. Department of health and human services. Web california medicaid management information system division ms 4727, p.o. Enclosed is the form, instructions for completing it, and where to return. They must also attach any bill ( s) they received from providers/suppliers. Get medicare forms for different situations, like filing a claim or appealing a coverage decision.
Ad download or email cms 1490s & more fillable forms, register and subscribe now! Web a cms 1490s form will be used by the centers for medicare and medicaid services. Filing a claim when you get services and/or supplies (if your provider. Web california medicaid management information system division ms 4727, p.o. Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services), durable medical. This particular form is known as the patient’s request for medical payment form. Enclosed is the form, instructions for completing it, and where to return. They must also attach any bill ( s) they received from providers/suppliers. Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Get medicare forms for different situations, like filing a claim or appealing a coverage decision.
Filing a claim when you get services and/or supplies (if your provider. Upload, modify or create forms. Ad download or email cms 1490s & more fillable forms, register and subscribe now! Please send the completed claim form, your itemized bill, and any supporting documents to the appropriate medicare contractor and. Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web a cms 1490s form will be used by the centers for medicare and medicaid services. This particular form is known as the patient’s request for medical payment form. Make sure it’s filed no later than 1 full. Enclosed is the form, instructions for completing it, and where to return. Your bill does not have to be paid before you submitthis claim for.

COVID Test Insurance Reimbursement Bedford Research Foundation
Web a cms 1490s form will be used by the centers for medicare and medicaid services. Web 11 rows cms forms list. Please send the completed claim form, your itemized bill, and any supporting documents to the appropriate medicare contractor and. Upload, modify or create forms. Web medicare will pay you directly when you complete this form and attach an.
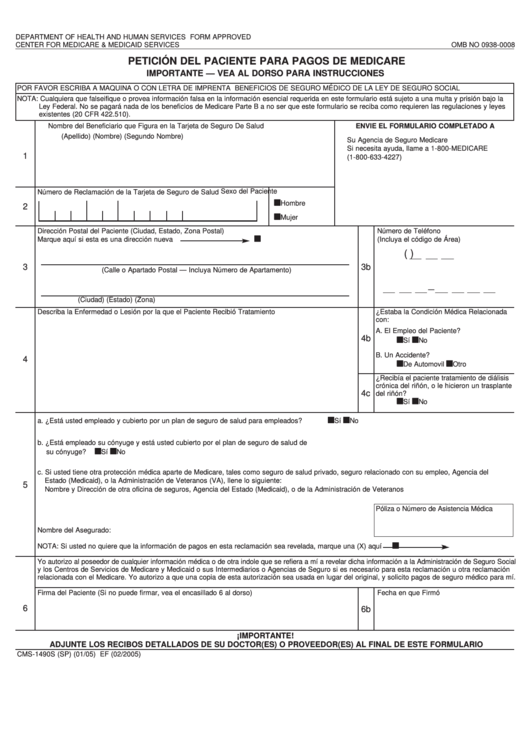
Form Cms1490s (Sp) Peticion Del Paciente Para Pagos De Medicare
Your bill does not have to be paid before you submitthis claim for. Ad download or email cms 1490s & more fillable forms, register and subscribe now! Web california medicaid management information system division ms 4727, p.o. Upload, modify or create forms. Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services),.
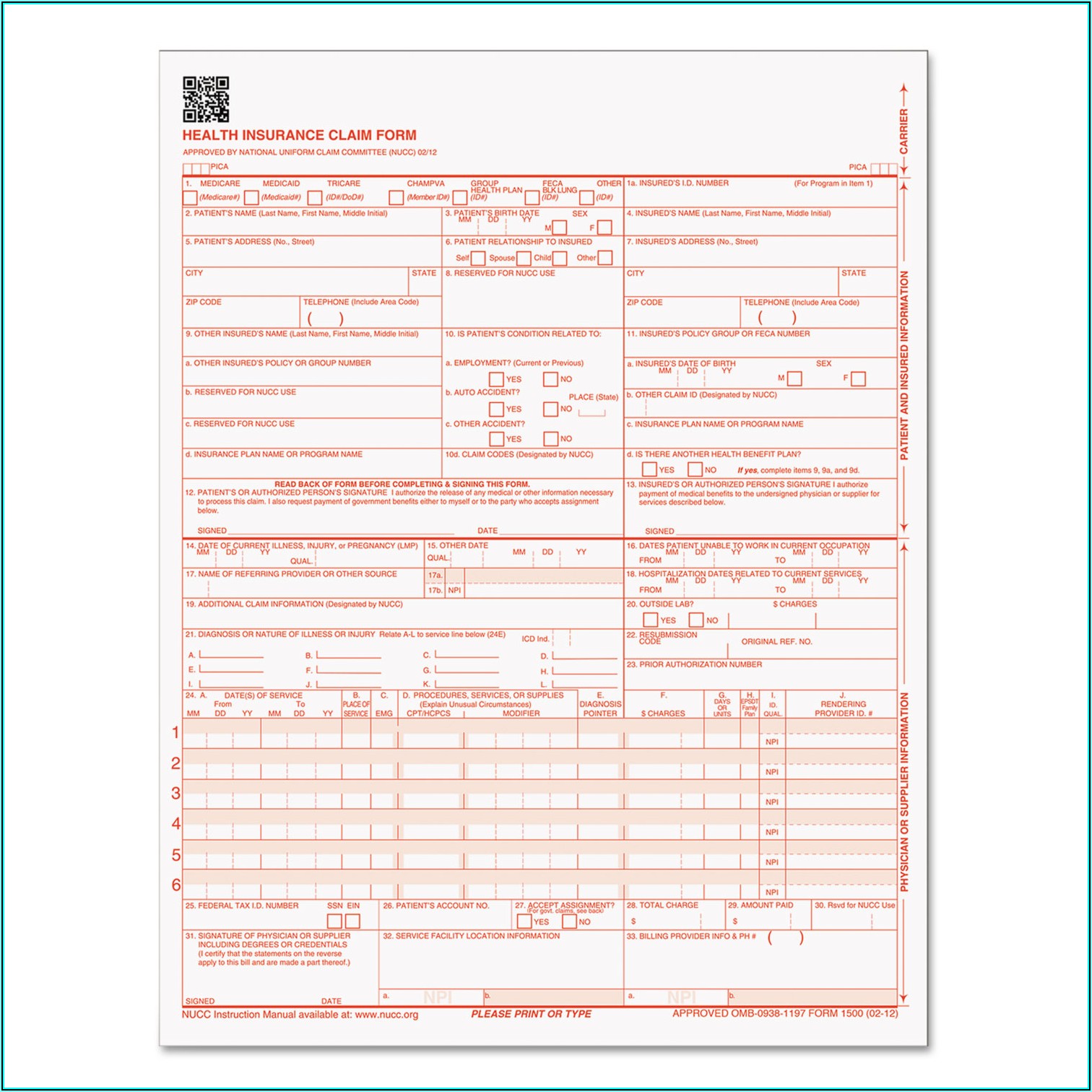
Medicare Cms 1500 Claim Form Form Resume Examples v19xkPk27E
Web 11 rows cms forms list. Make sure it’s filed no later than 1 full. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web (first) (middle) claim number from health insurance card send completed form to: Your bill does not have to be paid before you submitthis claim for.

Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Web 11 rows cms forms list. Enclosed is the form, instructions for completing it, and where to return. Department of health and human services. The following provides access and/or. Filing a claim when you get services and/or supplies (if your provider.
Medicare Form 1490s Dme Form Resume Examples XE8jblR8Oo
Ad download or email cms 1490s & more fillable forms, register and subscribe now! Make sure it’s filed no later than 1 full. The following provides access and/or. Web california medicaid management information system division ms 4727, p.o. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s.
Medicare Form 1490s Instructions Form Resume Examples Wk9yGWvV3D
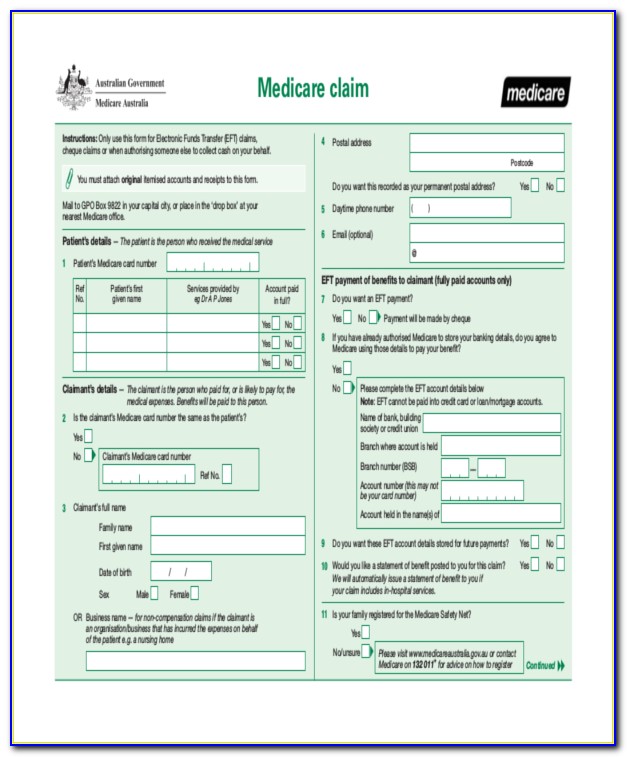
Web california medicaid management information system division ms 4727, p.o. Get medicare forms for different situations, like filing a claim or appealing a coverage decision. Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services), durable medical. Patient's request for medical payment: The following provides access and/or.
Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web a cms 1490s form will be used by the centers for medicare and medicaid services. Ad download or email cms 1490s & more fillable forms, register and subscribe now! Make sure it’s filed no.
Medicare Form 1490s Instructions Form Resume Examples Wk9yGWvV3D
Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services), durable medical. Web california medicaid management information system division ms 4727, p.o. Web 11 rows cms forms list. Upload, modify or create forms. Enclosed is the form, instructions for completing it, and where to return.
cms 1490s Fill out & sign online DocHub
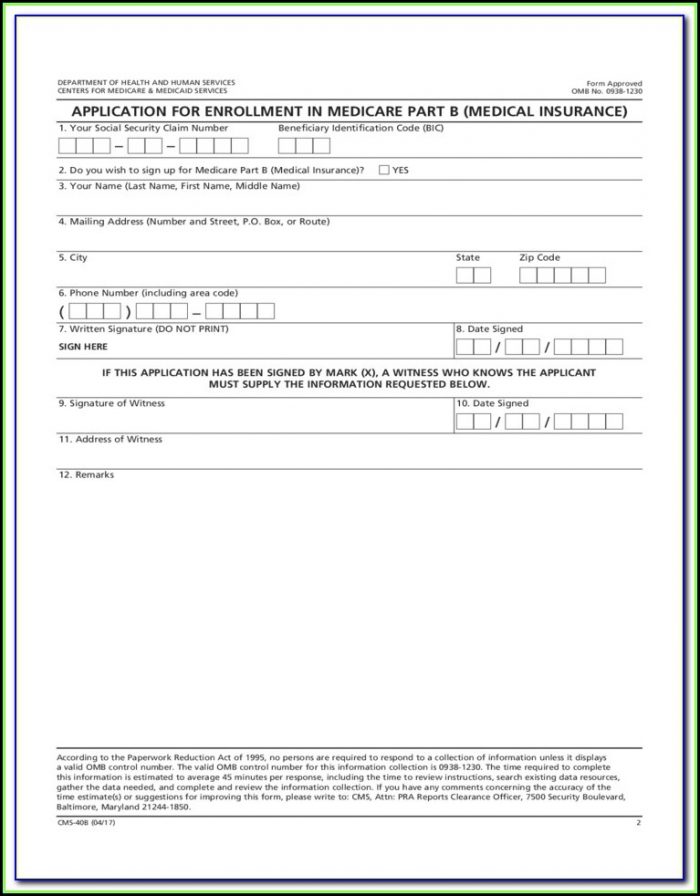
Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web if you need to file your own medicare claim, you’ll need to fill out a patient request for medical payment form, the 1490s. Department of health and human services. Ad download or email cms 1490s & more fillable forms, register and subscribe now!.
Medicare Claim Form 1490s Dme Form Resume Examples jNDAz4456x
Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Ad download or email cms 1490s & more fillable forms, register and subscribe now! Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web 11 rows cms forms.
Make Sure It’s Filed No Later Than 1 Full.
Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web a cms 1490s form will be used by the centers for medicare and medicaid services. Filing a claim when you get services and/or supplies (if your provider. The following provides access and/or.
Web Medicare Will Pay You Directly When You Complete This Form And Attach An Itemized Bill From Your Doctor Or Supplier.
Your bill does not have to be paid before you submitthis claim for. Get medicare forms for different situations, like filing a claim or appealing a coverage decision. Please send the completed claim form, your itemized bill, and any supporting documents to the appropriate medicare contractor and. Patient's request for medical payment:
This Particular Form Is Known As The Patient’s Request For Medical Payment Form.
Enclosed is the form, instructions for completing it, and where to return. They must also attach any bill ( s) they received from providers/suppliers. Department of health and human services. Upload, modify or create forms.
Web California Medicaid Management Information System Division Ms 4727, P.o.
Web patient’s request for medical payment for the influenza/pneumococcal vaccinations, part b services, (includes physician, laboratory, imaging services), durable medical. Web (first) (middle) claim number from health insurance card send completed form to: Web 11 rows cms forms list. Ad download or email cms 1490s & more fillable forms, register and subscribe now!