Meridian Pcp Change Form
Meridian Pcp Change Form - Failure to provide all required information. Am i eligible for the meridian medicaid plan? Web general what kind of health plan is meridianhealth? My health pays rewards® ways to save; Failure to provide all required information above will result in. Web primary care provider reassignment form pcp information member information *all fields containing an asterisk must be completed. Your provider will then send this. How do i contact meridian? Please complete this form with your provider if you want to change your pcp. Web you do not need to contact meridian for approval before receiving emergency services.
Web primary care provider reassignment form primary care provider (pcp) information member information all fields must be completed. Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Web general what kind of health plan is meridianhealth? About our coverage and benefits how much does it. Web primary care provider reassignment form primary care provider (pcp) information all fields must be completed. Web signature of member, parent, or the responsible party is requiredto approve pcp change form44 il fax completed primary care provider reassignment form to: Failure to provide all required information above will result in. Am i eligible for the meridian medicaid plan? Web we would like to show you a description here but the site won’t allow us. Web home our health plans show our health plans menu about our plans;
Web we would like to show you a description here but the site won’t allow us. Am i eligible to enroll in meridianhealth? If you don’t yet have a member account, visit member.ambetterhealth.com to set. Web primary care provider reassignment form pcp information member information *all fields containing an asterisk must be completed. Web signature of member, parent, or the responsible party is requiredto approve pcp change form44 il fax completed primary care provider reassignment form to: Please complete this form with your provider if you want to change your pcp. Failure to provide all information will. My health pays rewards® ways to save; Web general what kind of health plan is meridianhealth? Forms completed improperly or missing the member or responsible party signature will not be processed and the primary.

Pcp Change Request Form Template
How do i contact meridian? Web primary care provider reassignment form pcp information *all fields containing an asterisk must be completed. Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Web please select a form from the options below: If your situation is urgent but not life threatening, you should call.

MERIDIAN BIOSCIENCE INC FORM 8K EX99.1 EXHIBIT 99.1 March 23
If your situation is urgent but not life threatening, you should call your primary care. My health pays rewards® ways to save; Failure to provide all required information above will result in. A meridian pcp change form is a form that is used to change the designated primary care provider (pcp) for a patient in the. Web general what kind.

2021 TN BlueCare Primary Care Provider Change Request Form Fill Online
Web please select a form from the options below: Please complete this form with your provider if you want to change your pcp. Your provider will then send this. Cervical cancer screening exclusion form. Web primary care provider reassignment form primary care provider (pcp) information member information all fields must be completed.

Ching's Pediatrics Patient Forms Las Vegas, NV
Web general what kind of health plan is meridianhealth? Please complete this form with your provider if you want to change your pcp. About our coverage and benefits how much does it. Am i eligible for the meridian medicaid plan? Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be.
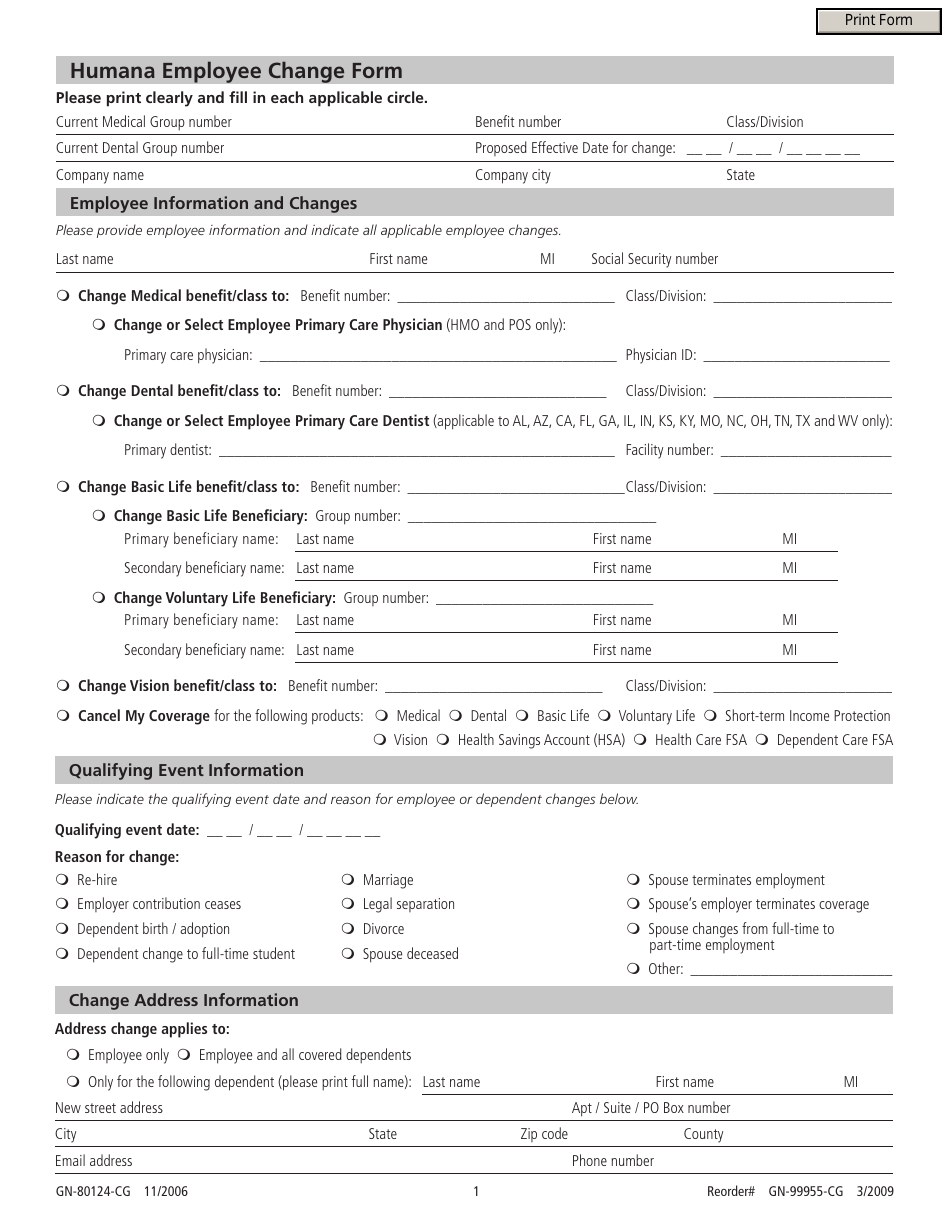
Form GN80124CG Download Fillable PDF or Fill Online Employee Change
Am i eligible for the meridian medicaid plan? Your provider will then send this. How do i contact meridian? Am i eligible to enroll in meridianhealth? Forms completed improperly or missing the member or responsible party signature will not be processed and the primary.
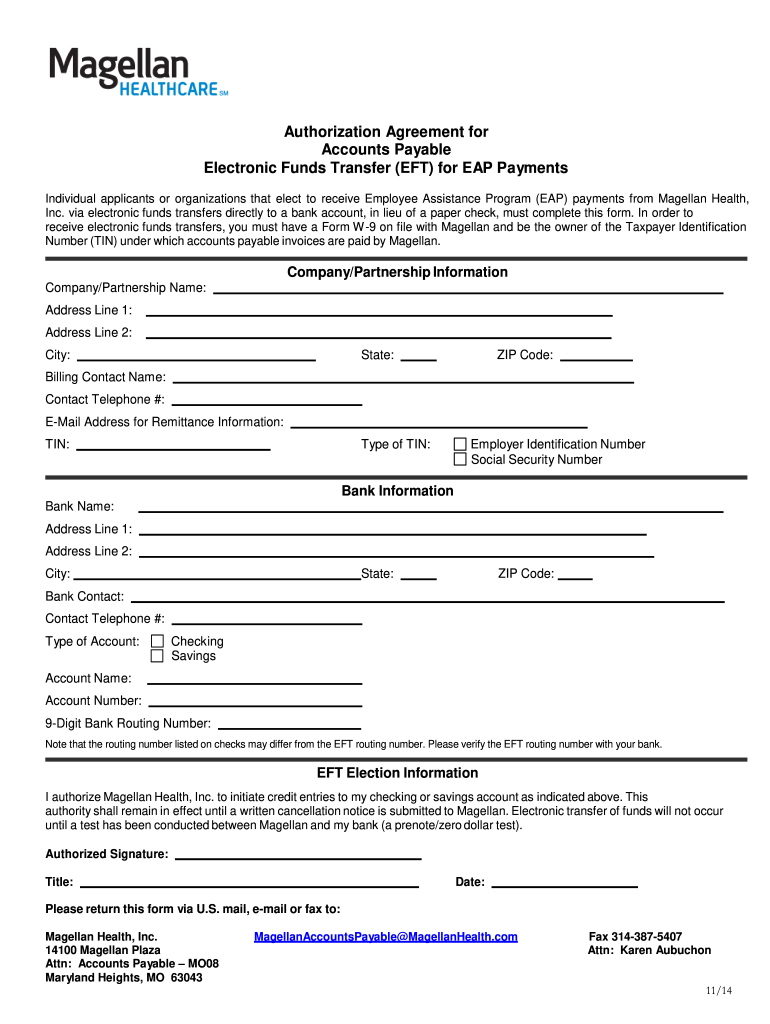
Magellan Eft Fill Out and Sign Printable PDF Template signNow
Web primary care provider reassignment form pcp information member information *all fields containing an asterisk must be completed. Web member primary care provider (pcp) change request form. Web breast cancer screening exclusion form. Web please select a form from the options below: Web you do not need to contact meridian for approval before receiving emergency services.

2008 Form DD 2876 Fill Online, Printable, Fillable, Blank pdfFiller
Failure to provide all required information above will result in. Web please select a form from the options below: Cervical cancer screening exclusion form. Web primary care provider reassignment form primary care provider (pcp) information all fields must be completed. Please complete this form with your provider if you want to change your pcp.

MeridianHSAElectionFormFillable1 Kleen Test Products Corporation
Am i eligible for the meridian medicaid plan? Am i eligible to enroll in meridianhealth? Learn how to help your patients keep their coverage. Web pharmacy provider resources for providers redetermination medicaid redetermination is here. Web you do not need to contact meridian for approval before receiving emergency services.

Highlevel PCP and patient behavior change algorithm. CPG clinical
Web please complete only one form per member household. What is the phone number and hours of operation for meridianhealth? About our coverage and benefits how much does it. Web meridian medicaid medical records. Web primary care provider reassignment form primary care provider (pcp) information member information all fields must be completed.

Aetna Facility Form Fill Online, Printable, Fillable, Blank pdfFiller
If you don’t yet have a member account, visit member.ambetterhealth.com to set. Forms completed improperly or missing the member or responsible party signature will not be processed and the primary. Web home our health plans show our health plans menu about our plans; Web general what kind of health plan is meridianhealth? Your provider will then send this.
Web Please Complete Only One Form Per Member Household.
How do i contact meridian? Web primary care provider reassignment form primary care provider (pcp) information all fields must be completed. Web you do not need to contact meridian for approval before receiving emergency services. About our coverage and benefits how much does it.
Web • Help Locating A Primary Care Provider (Pcp) • To Change Your Pcp • To Get Basic Plan Information • A New Meridiancomplete Id Card Or Handbook • To Change Your Address Or.
Web meridian medicaid medical records. Failure to provide all required information above will result in. Failure to provide all required information above will result in. Web primary care provider reassignment form primary care provider (pcp) information member information all fields must be completed.
Web Home Our Health Plans Show Our Health Plans Menu About Our Plans;
A meridian pcp change form is a form that is used to change the designated primary care provider (pcp) for a patient in the. Web primary care provider reassignment form pcp information *all fields containing an asterisk must be completed. Web we would like to show you a description here but the site won’t allow us. Web breast cancer screening exclusion form.
Web Member Primary Care Provider (Pcp) Change Request Form.
If you don’t yet have a member account, visit member.ambetterhealth.com to set. Cdc immunization schedules centers for disease control and prevention. Web what is a managed care plan? Your provider will then send this.