Patient Responsibility For Non Covered Services Form
Patient Responsibility For Non Covered Services Form - Web up to $40 cash back if you are a new user, click start free trial and establish a profile. Please retain this document in your patient’s medical record. Medical practitioner completing this form: Then upload your file to the system from your device,. This allows the claim to process and provide the. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Use the add new button. Web to render noncovered services to a patient, the provider should first make independent financial arrangements with the patient, acknowledging the patients'. I certify the above information to be true and accurate. Web • when considered patient responsibility, a waiver of liability may be required by the commercial plan.
Web oklahomadonotresuscitate (dnr) consent form i,, request limited health care as described in this document. I certify the above information to be true and accurate. Name (print) signature date of. The centers f or medicare & medicaid (cms) requires all medicare members, including dual eligible. If my heart stops beating or if i stop breathing, no medical. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Use the add new button. Medical practitioner completing this form: Please retain this document in your patient’s medical record. Web patient financial responsibility form 1.
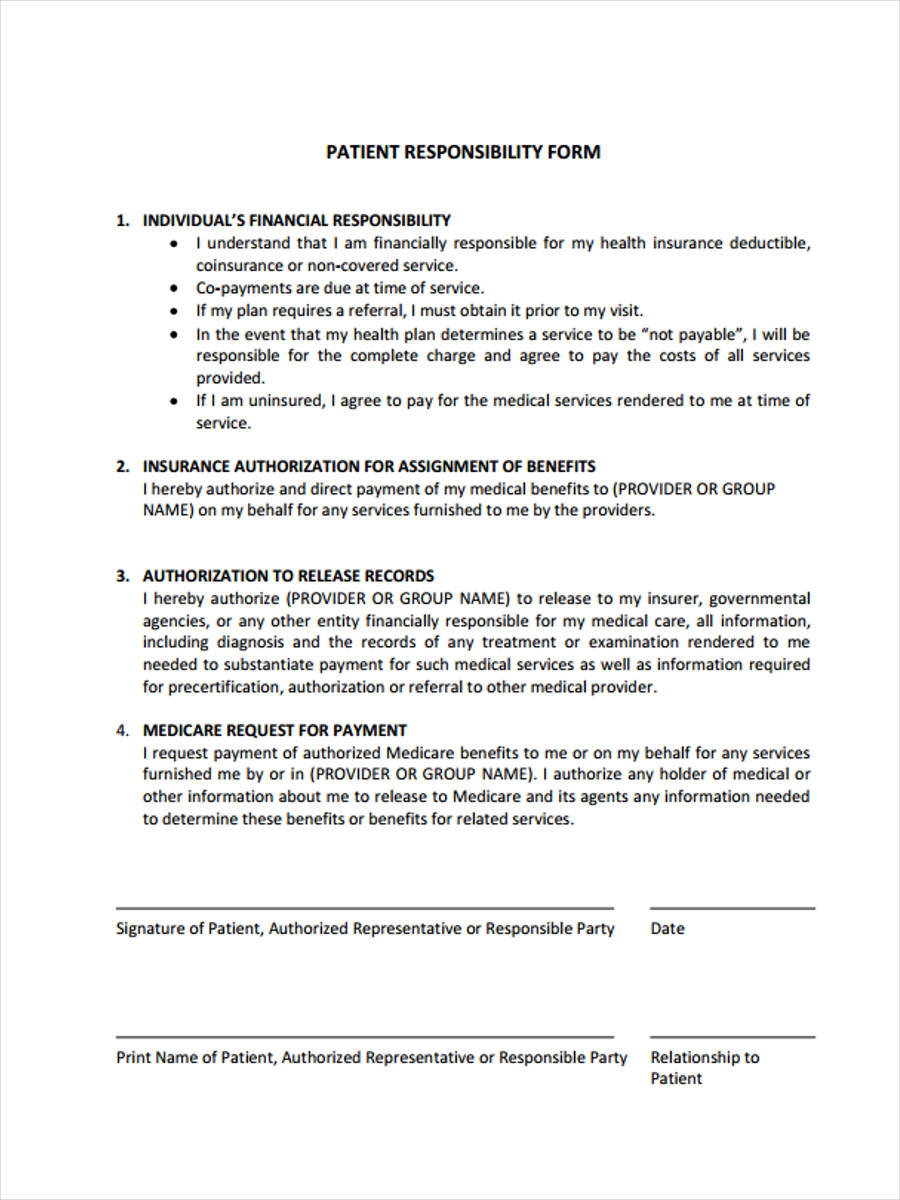
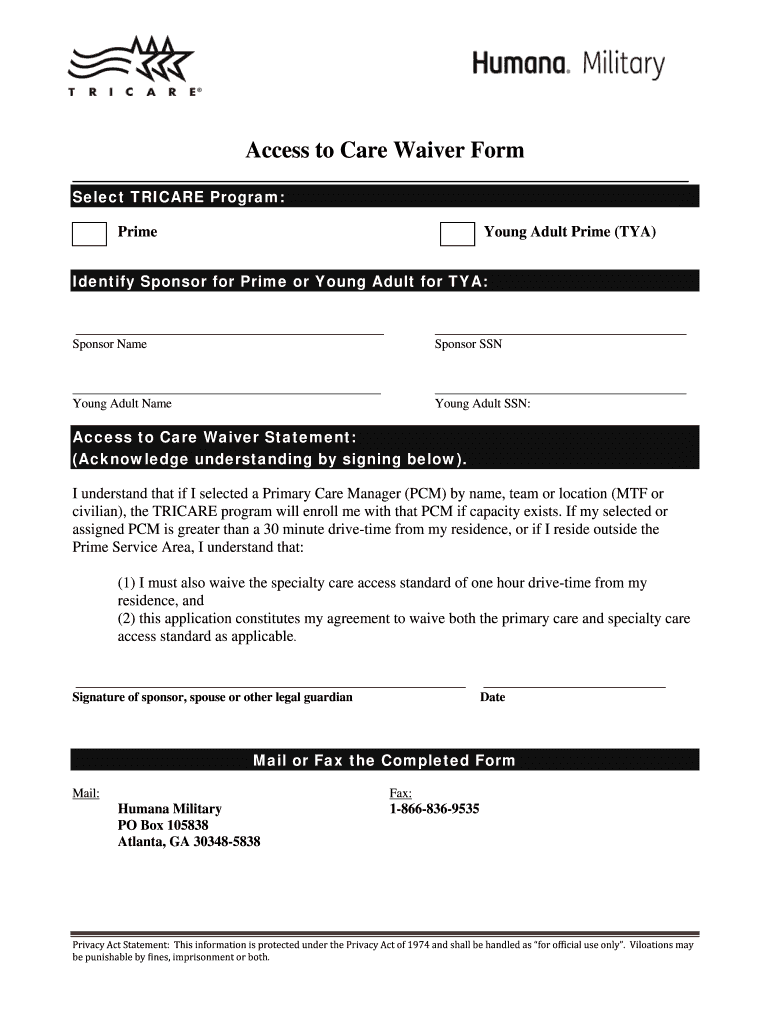
This allows the claim to process and provide the. Please retain this document in your patient’s medical record. Web patient financial responsibility form 1. Tricare or other governmental agencies may provide. Web up to $40 cash back if you are a new user, click start free trial and establish a profile. Then upload your file to the system from your device,. Use the add new button. Medical practitioner completing this form: Web oklahomadonotresuscitate (dnr) consent form i,, request limited health care as described in this document. Web • when considered patient responsibility, a waiver of liability may be required by the commercial plan.
FREE 8+ Financial Responsibility Forms in PDF Ms Word Excel
It would be considered not reasonable or. I certify the above information to be true and accurate. Web up to $40 cash back if you are a new user, click start free trial and establish a profile. Then upload your file to the system from your device,. Individual’s financial responsibility • i understand that i am financially responsible for my.
Tricare Non Covered Services Waiver Form Fill Out and Sign Printable
Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Web • when considered patient responsibility, a waiver of liability may be required by the commercial plan. Please retain this document in your patient’s medical record. Use the add.

A Guide to Running a Successful Patient Responsibility Pay Program
Please retain this document in your patient’s medical record. Web to render noncovered services to a patient, the provider should first make independent financial arrangements with the patient, acknowledging the patients'. Name (print) signature date of. If my heart stops beating or if i stop breathing, no medical. Tricare or other governmental agencies may provide.
Patients rights and responsibilities
Tricare or other governmental agencies may provide. Medical practitioner completing this form: Then upload your file to the system from your device,. The centers f or medicare & medicaid (cms) requires all medicare members, including dual eligible. Use the add new button.
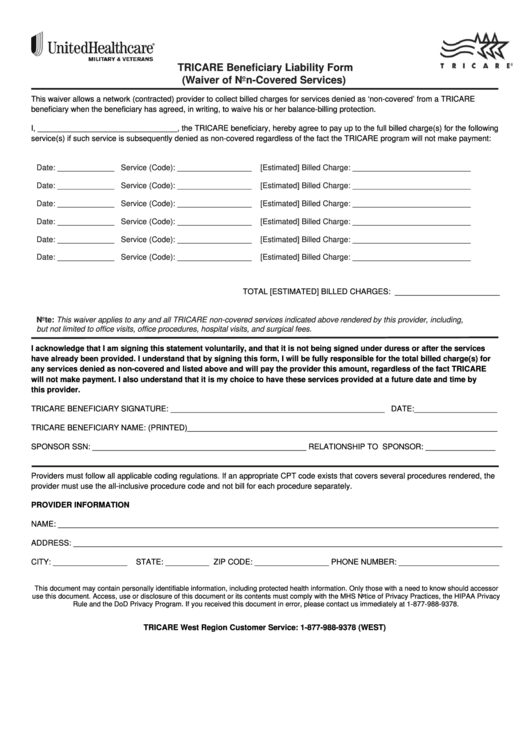
Fillable Tricare Beneficiary Liability Form (Waiver Of NonCovered
This allows the claim to process and provide the. Then upload your file to the system from your device,. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Tricare or other governmental agencies may provide. Web • when.

Patient Responsibility Labels, YOUR INSURANCE COMPANY... Fl Pink, 31
Use the add new button. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Then upload your file to the system from your device,. Web patient financial responsibility form 1. I certify the above information to be true.
PPT Allergy Immunotherapy in the College Health Setting PowerPoint
This allows the claim to process and provide the. Web patient financial responsibility form 1. Web • when considered patient responsibility, a waiver of liability may be required by the commercial plan. Individual’s financial responsibility • i understand that i am financially responsible for my health. Web up to $40 cash back if you are a new user, click start.
Medical Insurance Resolution & Patient Responsibility Services
Please retain this document in your patient’s medical record. Web oklahomadonotresuscitate (dnr) consent form i,, request limited health care as described in this document. I certify the above information to be true and accurate. Use the add new button. Web up to $40 cash back if you are a new user, click start free trial and establish a profile.
Patient Responsibility Due To Label 3 1/4" x 1 3/4" Fl Red MAP4180
Then upload your file to the system from your device,. Web up to $40 cash back if you are a new user, click start free trial and establish a profile. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable.

Healthcare Patient Responsibility Why the Costs Are Rising, and What
Web oklahomadonotresuscitate (dnr) consent form i,, request limited health care as described in this document. Individual’s financial responsibility • i understand that i am financially responsible for my health. Medical practitioner completing this form: Please retain this document in your patient’s medical record. If my heart stops beating or if i stop breathing, no medical.
Web To Render Noncovered Services To A Patient, The Provider Should First Make Independent Financial Arrangements With The Patient, Acknowledging The Patients'.
It would be considered not reasonable or. Tricare or other governmental agencies may provide. Then upload your file to the system from your device,. Medical practitioner completing this form:
Individual’s Financial Responsibility • I Understand That I Am Financially Responsible For My Health.
The centers f or medicare & medicaid (cms) requires all medicare members, including dual eligible. If my heart stops beating or if i stop breathing, no medical. Web medicare does not cover items and services unless the item or service is a defined benefit (section 1861 of the social security act), not statutorily excluded, and is reasonable and. Use the add new button.
Web • When Considered Patient Responsibility, A Waiver Of Liability May Be Required By The Commercial Plan.
Web patient financial responsibility form 1. I certify the above information to be true and accurate. This allows the claim to process and provide the. Web up to $40 cash back if you are a new user, click start free trial and establish a profile.
Web Oklahomadonotresuscitate (Dnr) Consent Form I,, Request Limited Health Care As Described In This Document.
Name (print) signature date of. Please retain this document in your patient’s medical record.