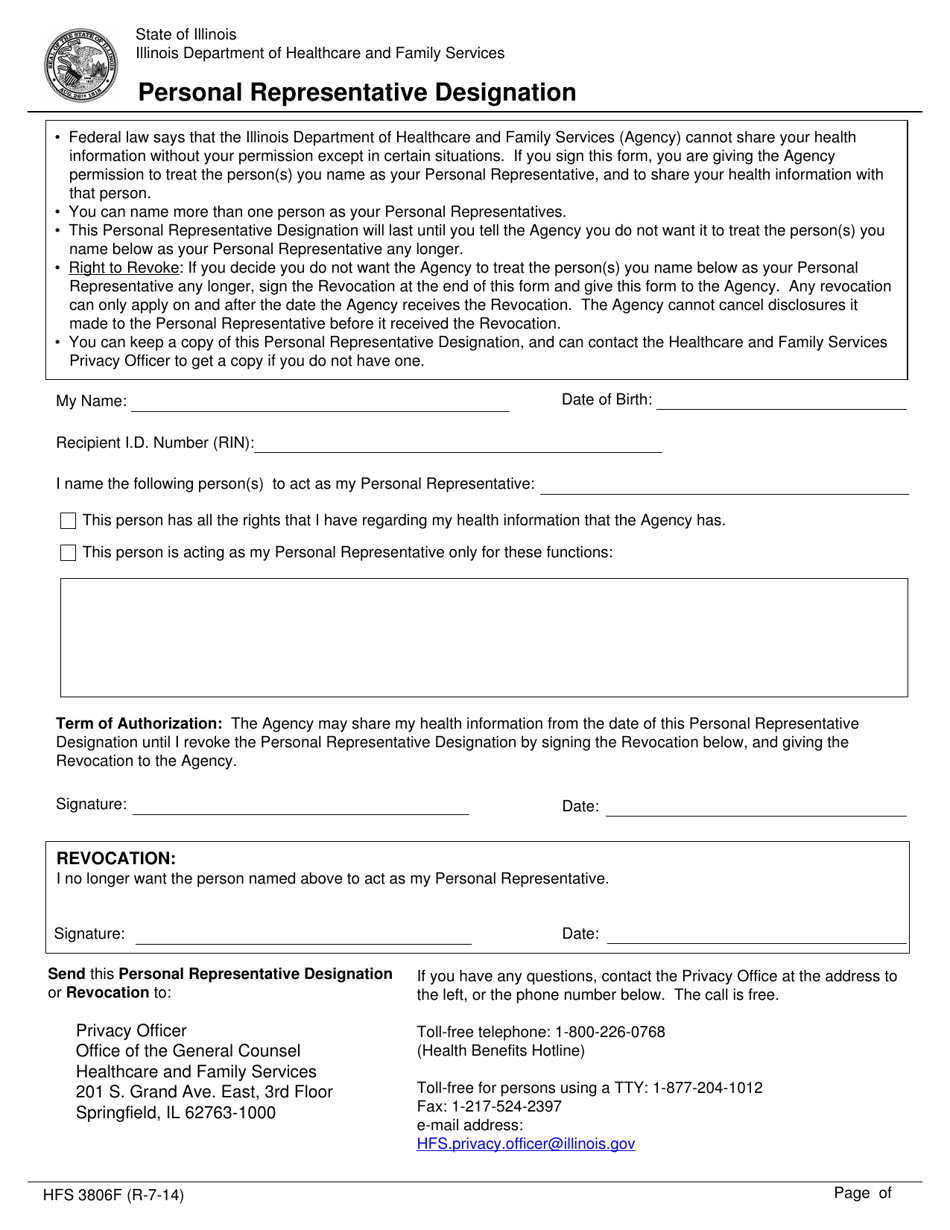
Personal Representative Designation Form
Personal Representative Designation Form - Web mail or fax the completed form and supporting documentation to: Give permission for us to talk to and share your health information with someone other than you or end. This person has all the rights that i have regarding my. Print, sign and bring your completed form to your. Web legal guardianis signing this form on behalf of the individual, please provide a copy of. Legal guardianis signing this form on be. Upmc personal representative designation form get. This form identifies a person who has legal authority to act on a member's behalf in making decisions. We understand that you wish to appoint a personal representative to act on your behalf as described below. This form tells us that you have named this person as your authorized personal representative.
Name the following person(s) to act as my personal representative: Privacy officer, colorado department of health care policy & financing 1570 grant street, denver, co 80203, fax: Web personal representative designation form dear patient: Web personal representative designation (prd) form (pdf): This person has all the rights that i have regarding my. Legal guardianis signing this form on be. This form tells us that you have named this person as your authorized personal representative. Fax your completed personal representative designation form. Your dependents over the age of 13 must complete, sign, and date a prd form to give upmc health plan permission. Web a personal representative may act on behalf of the patient for the purpose of receiving information that otherwise would be given to the patient.
Web personal representative designation form dear patient: This person has all the rights that i have regarding my. Upmc personal representative designation form get. Web return completed form to: Web what is a personal representative designation form? Web use the personal representative designation form to: Fax your completed personal representative designation form. Web up to 8% cash back to designate or remove your personal representative, please download the necessary forms below. This form tells us that you have named this person as your authorized personal representative. Your dependents over the age of 13 must complete, sign, and date a prd form to give upmc health plan permission.

Authorized Representative Designation Form Masshealth
Give permission for us to talk to and share your health information with someone other than you or end. This person has all the rights that i have regarding my. Web designation of personal representative. Name the following person(s) to act as my personal representative: Upmc personal representative designation form get.
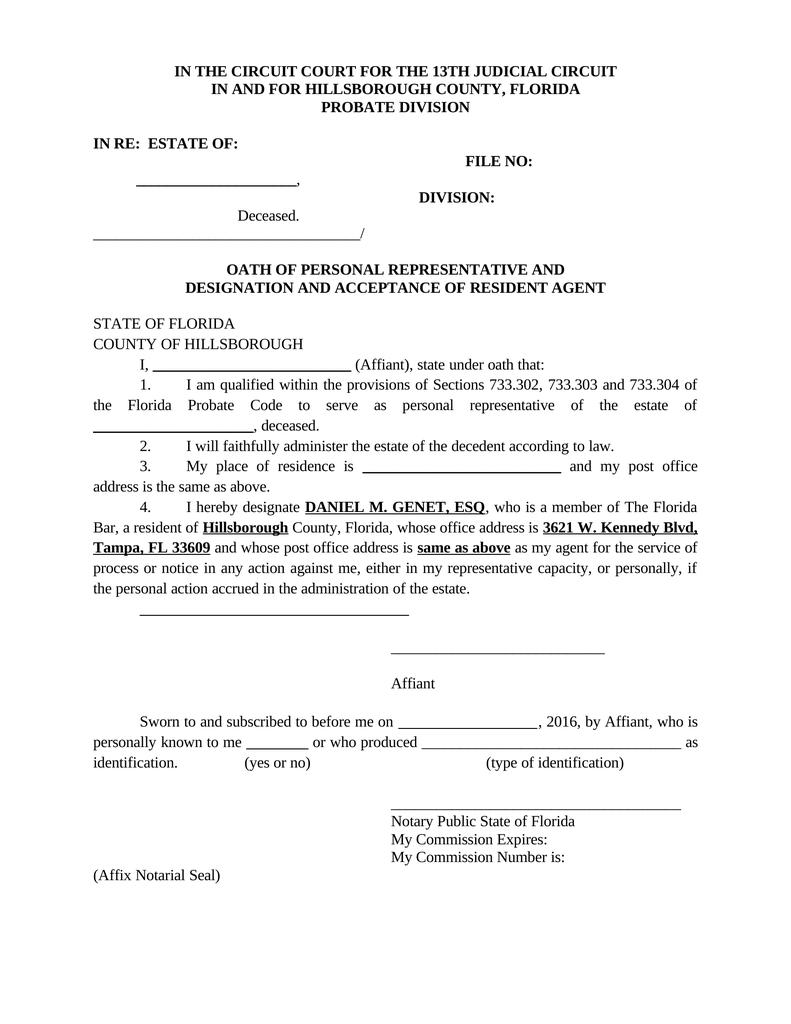
Oath of Personal Representative & Designation & Acceptance of Resident
Web personal representative designation (prd) form (pdf): Web you may designate a personal representative who will act on your behalf in making decisions related to health care, which includes treatment and payment issues. Web designation of personal representative. Download, print, fill out, and sign the personal representative designation form b. We understand that you wish to appoint a personal representative.
Form HFS3806F Download Fillable PDF or Fill Online Personal
Your dependents over the age of 13 must complete, sign, and date a prd form to give upmc health plan permission. Web designation of personal representative. Web when a personal representative is being designated by a customer, the customer needs to sign this form in the presence of a notary public. Web designate a personal representative if you would like.
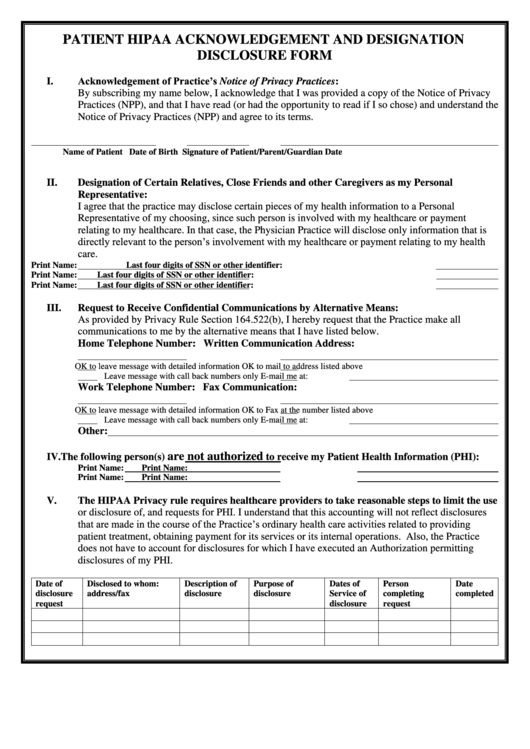
Patient Hipaa Acknowledgement And Designation Disclosure Form printable
Web designation of personal representative. Web personal representative designation form dear patient: Web designate a personal representative if you would like another person to act on your behalf when discussing your health care coverage and benefit information, you will need. Print, sign and bring your completed form to your. You can limit the amount of information that the authorized personal.

AllWays Health Partners Authorized Personal Representative Designation
Download, print, fill out, and sign the personal representative designation form b. Web designation of personal representative. We understand that you wish to appoint a personal representative to act on your behalf as described below. “dartmouth health (dh)” is the corporate parent of the covered entities listed below, each of which is an individual. Privacy officer, colorado department of health.
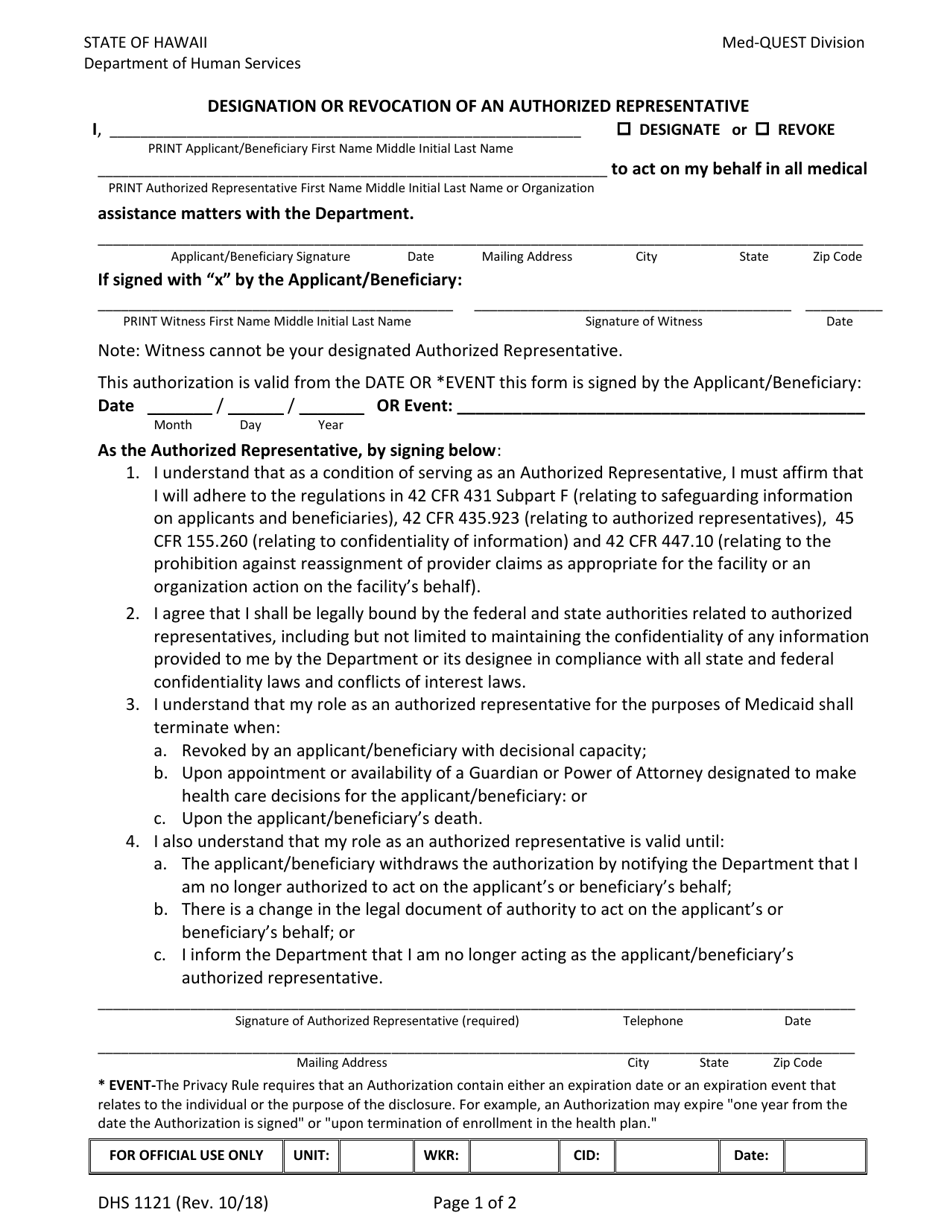
Form DHS1121 Download Fillable PDF or Fill Online Designation or
Web designation of personal representative. Print, sign and bring your completed form to your. Web return completed form to: Web up to 8% cash back to designate or remove your personal representative, please download the necessary forms below. You can limit the amount of information that the authorized personal.
Appointed Representative Agreement Template
Web designate a personal representative if you would like another person to act on your behalf when discussing your health care coverage and benefit information, you will need. Give permission for us to talk to and share your health information with someone other than you or end. Your dependents over the age of 13 must complete, sign, and date a.
MEBA Medical Plan Designation of Authorized Representative Form Fill
Web designate a personal representative if you would like another person to act on your behalf when discussing your health care coverage and benefit information, you will need. Web legal guardianis signing this form on behalf of the individual, please provide a copy of. Print, sign and bring your completed form to your. Web use the personal representative designation form.

Release and Indemnification of Personal Representative by Heirs and
Print, sign and bring your completed form to your. Give permission for us to talk to and share your health information with someone other than you or end. Web personal representative designation form dear patient: Web you may designate a personal representative who will act on your behalf in making decisions related to health care, which includes treatment and payment.
Top 15 Authorized Representative Form Templates free to download in PDF
Your dependents over the age of 13 must complete, sign, and date a prd form to give upmc health plan permission. Legal guardianis signing this form on be. This form identifies a person who has legal authority to act on a member's behalf in making decisions. Web you may designate a personal representative who will act on your behalf in.
“Dartmouth Health (Dh)” Is The Corporate Parent Of The Covered Entities Listed Below, Each Of Which Is An Individual.
Web designation of personal legal representative. Web when a personal representative is being designated by a customer, the customer needs to sign this form in the presence of a notary public. Web personal representative designation (prd) form (pdf): This form tells us that you have named this person as your authorized personal representative.
We Understand That You Wish To Appoint A Personal Representative To Act On Your Behalf As Described Below.
Print, sign and bring your completed form to your. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your. You can limit the amount of information that the authorized personal. This person has all the rights that i have regarding my.
Web Up To 8% Cash Back To Designate Or Remove Your Personal Representative, Please Download The Necessary Forms Below.
Web what is a personal representative designation form? Legal guardianis signing this form on be. Web return completed form to: Upmc personal representative designation form get.
Web Designate A Personal Representative If You Would Like Another Person To Act On Your Behalf When Discussing Your Health Care Coverage And Benefit Information, You Will Need.
Give permission for us to talk to and share your health information with someone other than you or end. Web personal representative designation form dear patient: Privacy officer, colorado department of health care policy & financing 1570 grant street, denver, co 80203, fax: Fax your completed personal representative designation form.