Redetermination Form Medicare
Redetermination Form Medicare - Web a redetermination must be requested in writing. Web if you received your redetermination notice more than 180 days ago, include your reason for the late filing: Web medicare part b redetermination form is a document that your doctor must fill out when you are admitted to a facility for more than ninety days. Your name and medicare number. Item or service you wish to. Web medicare redetermination request form — 1st level of appeal. Beneficiary’s name (first, middle, last) medicare number. Web view redetermination or reopening form tutorial for completion assistance. Web submitting redetermination requests. A claim must be appealed within 120 days.
Beneficiary’s name (first, middle, last) medicare number. Item or service you wish to. Web redetermination/reopening form instructions. Your name and medicare number. Web a redetermination is the first level of an appeal and is a request to review a claim when there is a dissatisfaction with the original determination. A redetermination is the first level of the. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. A claim must be appealed within 120 days. Your next level of appeal is a reconsideration by a. A claim must be appealed within 120 days.
Web a redetermination is the first level of an appeal and is a request to review a claim when there is a dissatisfaction with the original determination. Your name and medicare number. Note that data items are in groups of related information. This form may be used to request a redetermination for medicare part b services. Beneficiary’s name (first, middle, last) medicare number. A redetermination is the first level of the. Web fill out a medicare reconsideration request form. [pdf, 180 kb] submit a written request to the qic that includes: Web medicare part b redetermination form is a document that your doctor must fill out when you are admitted to a facility for more than ninety days. Please submit a new claim with the. Web view redetermination or reopening form tutorial for completion assistance.
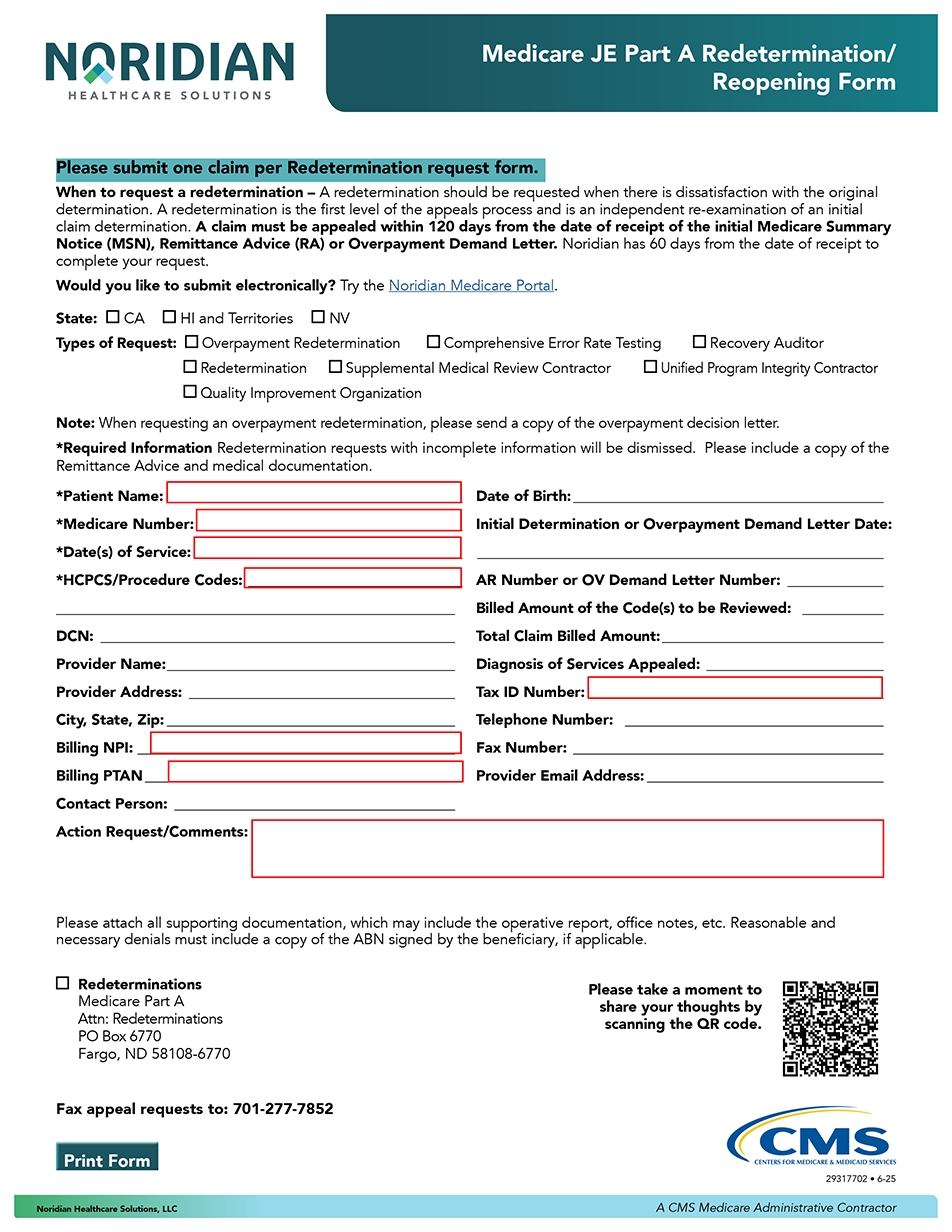
Redetermination/Reopening Form Tutorial JE Part A Noridian
A claim must be appealed within 120 days. Web a redetermination is the first level of an appeal and is a request to review a claim when there is a dissatisfaction with the original determination. Web submitting redetermination requests. Web first level appeal (redetermination) an appeal is a new and independent examination of a claim due to dissatisfaction of the.
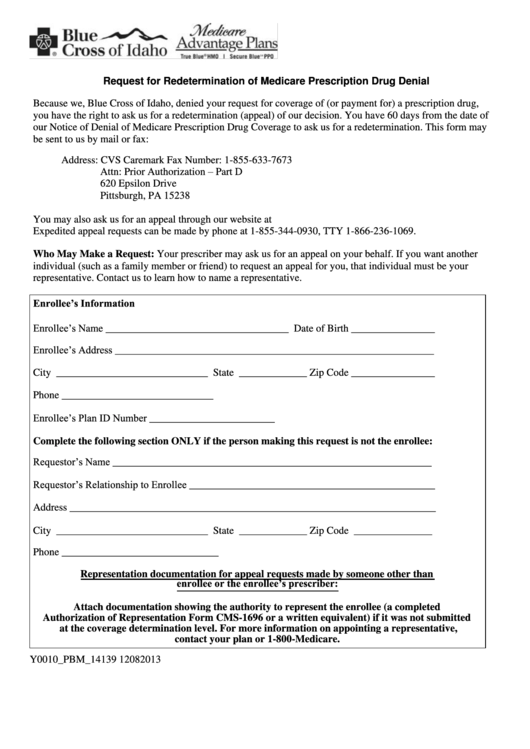
Request For Redetermination Of Medicare Prescription Drug Denial
Send completed form and any applicable medical documentation (may include the. Web fill out a redetermination request form [pdf, 100 kb] and send it to the medicare contractor at the address listed on the msn. Web a redetermination is the first level of an appeal and is a request to review a claim when there is a dissatisfaction with the.
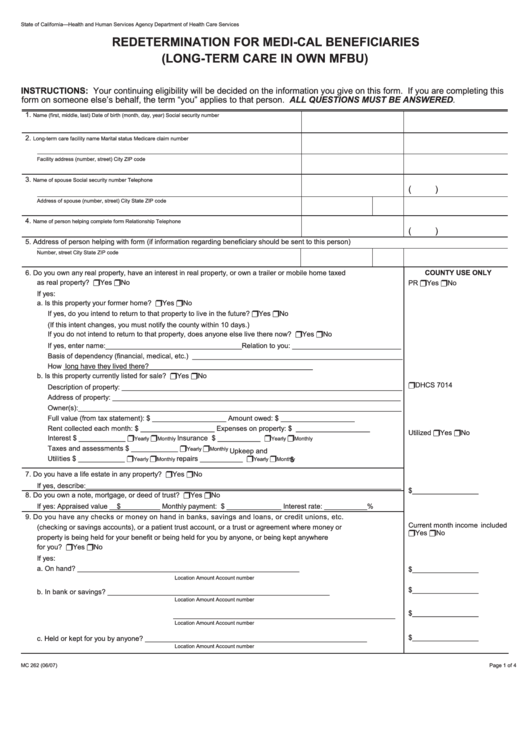
Fillable Form Mc 262 Redetermination For MediCal Beneficiaries (Long
Web first level appeal (redetermination) an appeal is a new and independent examination of a claim due to dissatisfaction of the initial claim determination. Web an enrollee, an enrollee's representative, or an enrollee's prescriber may use this model form to request a redetermination (appeal) from a plan sponsor. Beneficiary’s name (first, middle, last) medicare number. Your next level of appeal.

DA Request For Redetermination of Medicare Prescription Drug Denial
Web paper form completion instructions are provided for each data item, which is indicated by a number. Web a redetermination must be requested in writing. Web medicare redetermination request form — 1st level of appeal. Note that data items are in groups of related information. Web if you received your redetermination notice more than 180 days ago, include your reason.
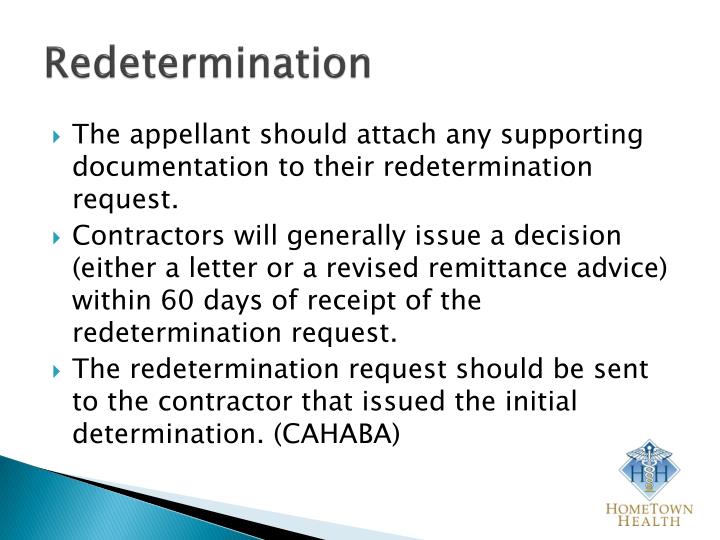
PPT THE MEDICARE APPEALS PROCESS PowerPoint Presentation ID6195200
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web fill out a medicare reconsideration request form. [pdf, 180 kb] submit a written request to the qic that includes: Web first level appeal (redetermination) an appeal is a new and independent examination of a claim due to dissatisfaction of.
Redetermination Fill Out and Sign Printable PDF Template signNow
Web medicare part b redetermination form is a document that your doctor must fill out when you are admitted to a facility for more than ninety days. Your next level of appeal is a reconsideration by a. Web medicare redetermination request form — 1st level of appeal. Web an enrollee, an enrollee's representative, or an enrollee's prescriber may use this.
Form Cms20027 Medicare Redetermination Request Form, Form Cms20034
Web fill out a medicare reconsideration request form. [pdf, 180 kb] submit a written request to the qic that includes: Beneficiary’s name (first, middle, last) medicare number. Web a redetermination must be requested in writing. Send completed form and any applicable medical documentation (may include the. If questions arise when completing a redetermination/reopening form, please see the below.

Medicare part b redetermination form 2019 Fill out & sign online DocHub
Web redetermination/reopening form instructions. This form may be used to request a redetermination for medicare part b services. Web medicare redetermination request form — 1st level of appeal. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web view redetermination or reopening form tutorial for completion assistance.
Medicare Savings Programs Application/redetermination (Qmb, Slmb, Almb
A claim must be appealed within 120 days. This form may be used to request a redetermination for medicare part b services. Web submitting redetermination requests. Web a redetermination must be requested in writing. If questions arise when completing a redetermination/reopening form, please see the below.

Example Medicare redetermination form Medicare Payment, Reimbursement
Web redetermination/reopening form instructions. Web medicare redetermination request form — 1st level of appeal. Web a redetermination is the first level of an appeal and is a request to review a claim when there is a dissatisfaction with the original determination. Your name and medicare number. Note that data items are in groups of related information.
Your Name And Medicare Number.
Item or service you wish to. A claim must be appealed within 120 days. Web redetermination/reopening form instructions. Please submit a new claim with the.
Web Submitting Redetermination Requests.
If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. A claim must be appealed within 120 days. Your next level of appeal is a reconsideration by a. This form may be used to request a redetermination for medicare part b services.
Send Completed Form And Any Applicable Medical Documentation (May Include The.
Requesting an appeal (redetermination) if you disagree with. Web medicare part b redetermination form is a document that your doctor must fill out when you are admitted to a facility for more than ninety days. If questions arise when completing a redetermination/reopening form, please see the below. Web a redetermination must be requested in writing.
Follow The Instructions For Sending An.
Web first level appeal (redetermination) an appeal is a new and independent examination of a claim due to dissatisfaction of the initial claim determination. Web fill out a medicare reconsideration request form. [pdf, 180 kb] submit a written request to the qic that includes: Web an enrollee, an enrollee's representative, or an enrollee's prescriber may use this model form to request a redetermination (appeal) from a plan sponsor. Web medicare redetermination request form — 1st level of appeal.