Voya Hospital Indemnity Claim Form
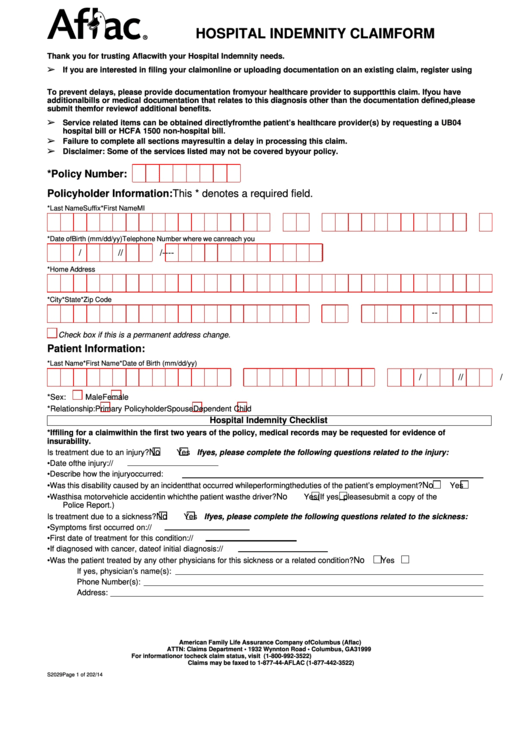
Voya Hospital Indemnity Claim Form - Po box 320, minneapolis, mn 55440 overnight address: Web submit at voya.com/claims(select upload documents) phone: Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays. Web file a dental claim via fax or mail. Attach a copy of the hospital itemized bill (hospital form ub04) and/or. Web voya claim , voya claims , voya insurance claim , voya insurance claims , voya employee benefits claims , voya employee benefit claim Web employees enrolled in accident insurance or hospital indemnity insurance can file a claim online without having to print and sign forms to upload. Web submit at voya.com/claims (select upload documents) phone: Web 1 based on 2018 data from the u.s. The benefit amount is determined.
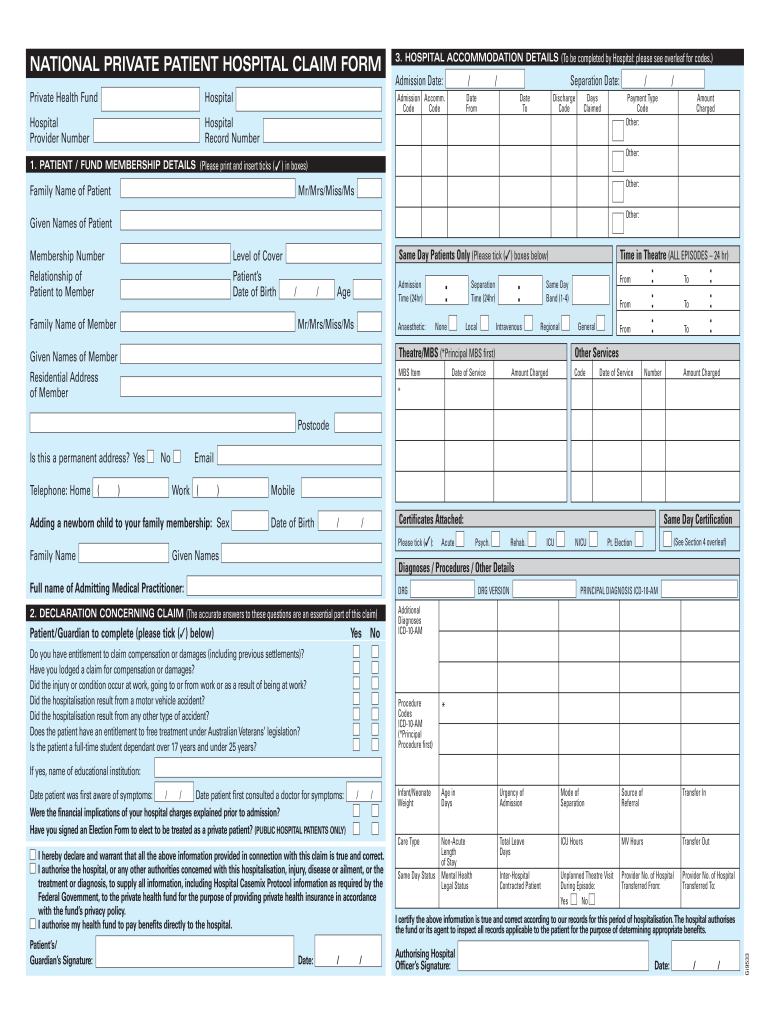
The benefit amount is determined by. An attending physicians statement of hospital confinement indeminity form (available in the forms library), indicating the. Attach a copy of the hospital itemized bill (hospital form ub04) and/or. Web insurance, and hospital indemnity insurance. Web file a dental claim via fax or mail. Web hospital confinement indemnity insurance pays a daily benefit if you have a covered stay in a hospital*, critical care unit or rehabilitation facility. Po box 320, minneapolis, mn 55440 overnight address: As you explore, keep in mind: Web accident c hospital confinement indemnity c critical illness / specified disease submit at voya.com (select contact & services > claims center > upload a. Principal life insurance company attn:
Web voya claim , voya claims , voya insurance claim , voya insurance claims , voya employee benefits claims , voya employee benefit claim As you explore, keep in mind: Web 1 based on 2018 data from the u.s. An attending physicians statement of hospital confinement indeminity form (available in the forms library), indicating the. Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays. Web file a dental claim via fax or mail. Disability claim form instructions, employer and employee statements (pdf). Agency for healthcare research and quality's medical expenditure survey 2 american journal of public health, medical bankruptcy: Hit enter to return to the slide. Web a completed hospital indemnity claim form:
Aarp Hospital Indemnity Plan Claim Form
Web submit at voya.com/claims(select upload documents) phone: Web 1 based on 2018 data from the u.s. Po box 320, minneapolis, mn 55440 overnight address: Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays. Attach a copy of the hospital itemized bill (hospital form ub04) and/or.

voya claimant statement Fill out & sign online DocHub
Web hospital confinement indemnity insurance pays a daily benefit if you have a covered stay in a hospital*, critical care unit or rehabilitation facility. The benefit amount is determined by. Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays. Po box 320, minneapolis, mn 55440 overnight address: Web claim checklist sign and.
Top 52 Aflac Forms And Templates free to download in PDF format
Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays. The benefit amount is determined. Web file a dental claim via fax or mail. An attending physicians statement of hospital confinement indeminity form (available in the forms library), indicating the. Web insurance, and hospital indemnity insurance.
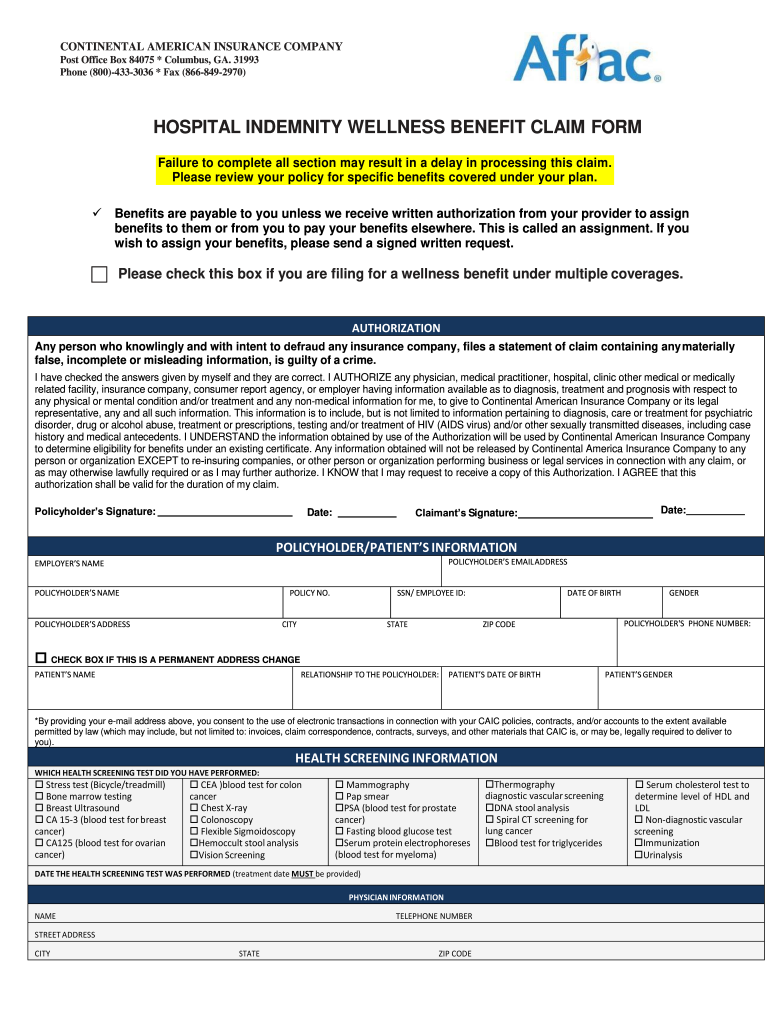
Hospital Indemnity Wellness Benefit Claim Form Aflac Group Insurance
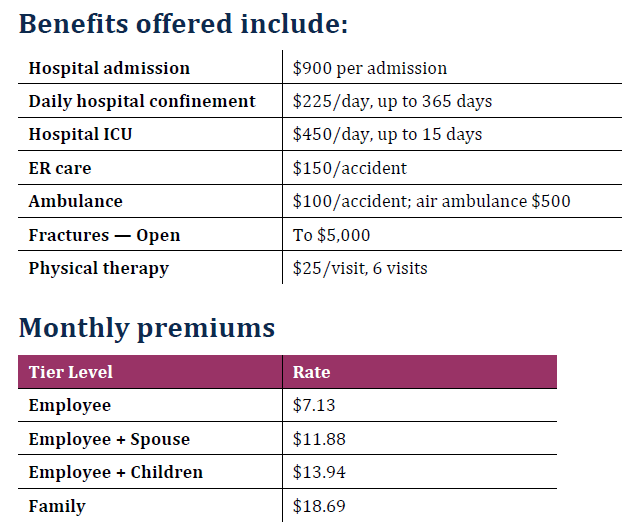
Web this document includes expanded cost and benefit information for hospital indemnity insurance. Attach a copy of the hospital itemized bill (hospital form ub04) and/or. Disability claim form instructions, employer and employee statements (pdf). Web hospital confinement indemnity insurance is underwritten by reliastar life insurance company (minneapolis, mn), a member of the voya® family of companies. Web 1 based on.
Voya Financial Annuity Claim Form Form Resume Examples Bw9jAbn27X
Web hospital confinement indemnity insurance pays a daily benefit if you have a covered stay in a hospital*, critical care unit or rehabilitation facility. As you explore, keep in mind: Agency for healthcare research and quality's medical expenditure survey 2 american journal of public health, medical bankruptcy: Web insurance, and hospital indemnity insurance. Web a completed hospital indemnity claim form:

Claim Form Hospital Patient
Depending on the plan, hospital indemnity. Hit enter to return to the slide. The benefit amount is determined. Web 1 based on 2018 data from the u.s. Web hospital indemnity insurance supplements your existing health insurance coverage by helping pay expenses for hospital stays.
Hc21 Form Fill Out and Sign Printable PDF Template signNow
Po box 320, minneapolis, mn 55440 overnight address: Web insurance, and hospital indemnity insurance. Web 1 based on 2018 data from the u.s. Web find the required forms and documents based on your state of residence for your voya® employee benefits insurance policies. Disability claim form instructions, employer and employee statements (pdf).

Aarp Hospital Indemnity Plan Claim Form
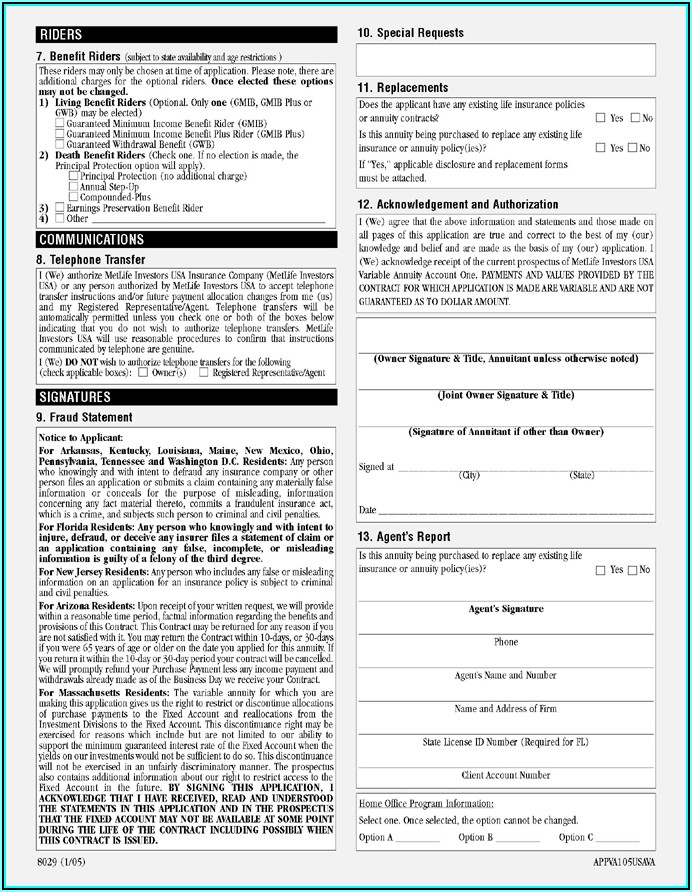
Disability claim form instructions, employer and employee statements (pdf). The benefit amount is determined by. For a complete description of your available benefits, exclusions and limitations, see your. Web find the required forms and documents based on your state of residence for your voya® employee benefits insurance policies. Web 1 based on 2018 data from the u.s.
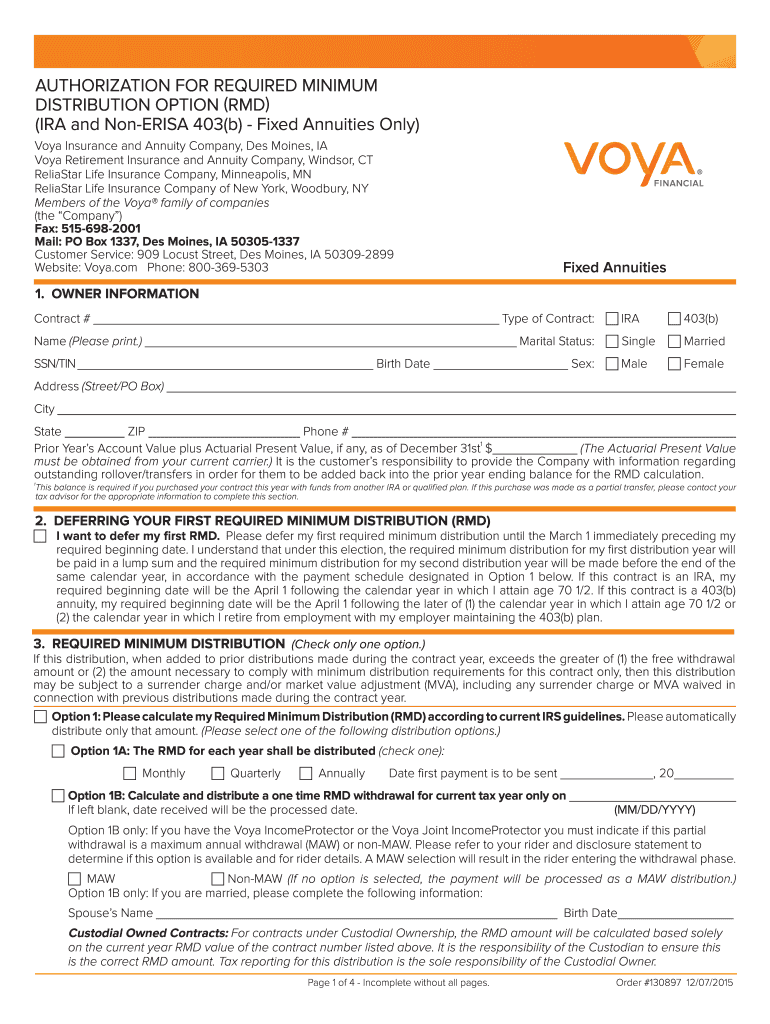
Required Minimum Distribution Voya for Professionals Fill Out and
Web hospital confinement indemnity insurance pays a daily benefit if you have a covered stay in a hospital*, critical care unit or rehabilitation facility. Po box 320, minneapolis, mn 55440 overnight address: Web employees enrolled in accident insurance or hospital indemnity insurance can file a claim online without having to print and sign forms to upload. Agency for healthcare research.
Voya Hospital Indemnity Insurance / Voya Claimant Statement 2015 Fill
No medical questions or tests are required for. Web find the required forms and documents based on your state of residence for your voya® employee benefits insurance policies. Po box 320, minneapolis, mn 55440 overnight address: Depending on the plan, hospital indemnity. Web insurance, and hospital indemnity insurance.
250 Marquette Ave., Suite 900,.
Web voya claim , voya claims , voya insurance claim , voya insurance claims , voya employee benefits claims , voya employee benefit claim Web 1 based on 2018 data from the u.s. Web claim checklist sign and date this completed form, then submit using one of the above methods. The benefit amount is determined by.
Web Submit At Voya.com/Claims(Select Upload Documents) Phone:
Web employees enrolled in accident insurance or hospital indemnity insurance can file a claim online without having to print and sign forms to upload. For a complete description of your available benefits, exclusions and limitations, see your. Web find the required forms and documents based on your state of residence for your voya® employee benefits insurance policies. Disability claim form instructions, employer and employee statements (pdf).
Agency For Healthcare Research And Quality's Medical Expenditure Survey 2 American Journal Of Public Health, Medical Bankruptcy:
As you explore, keep in mind: No medical questions or tests are required for. Hit enter to return to the slide. Web a completed hospital indemnity claim form:
Po Box 320, Minneapolis, Mn 55440 Overnight Address:
The benefit amount is determined. Attach a copy of the hospital itemized bill (hospital form ub04) and/or. Web hospital confinement indemnity insurance is underwritten by reliastar life insurance company (minneapolis, mn), a member of the voya® family of companies. Web online disability insurance claim form;