Form 1500 Claim
Form 1500 Claim - Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Web cms 1500 dynamic list information. Web the nucc does not process claims. You can decide how often to. Item 1a insured’s id number (patient’s medicare health insurance claim number. It can be purchased in any version required by calling the u.s. Web using cms form 1500/hcfa: • your current forms supplier; Do not email completed 1500 claim forms to the nucc. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy.
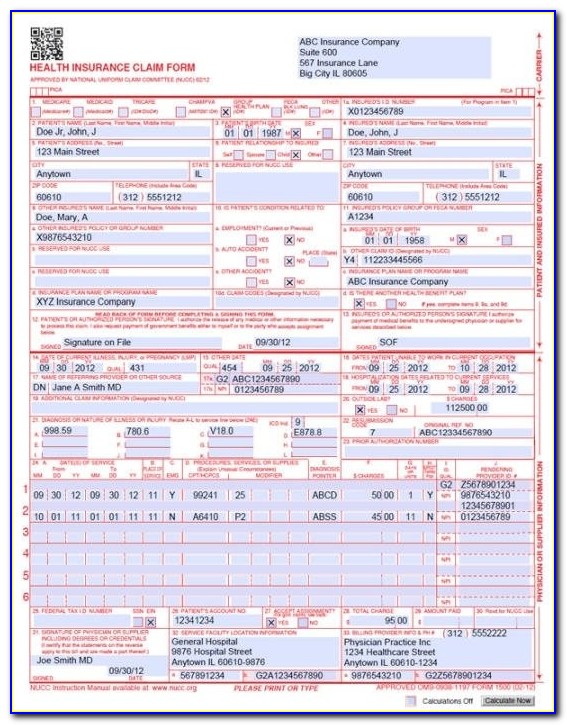
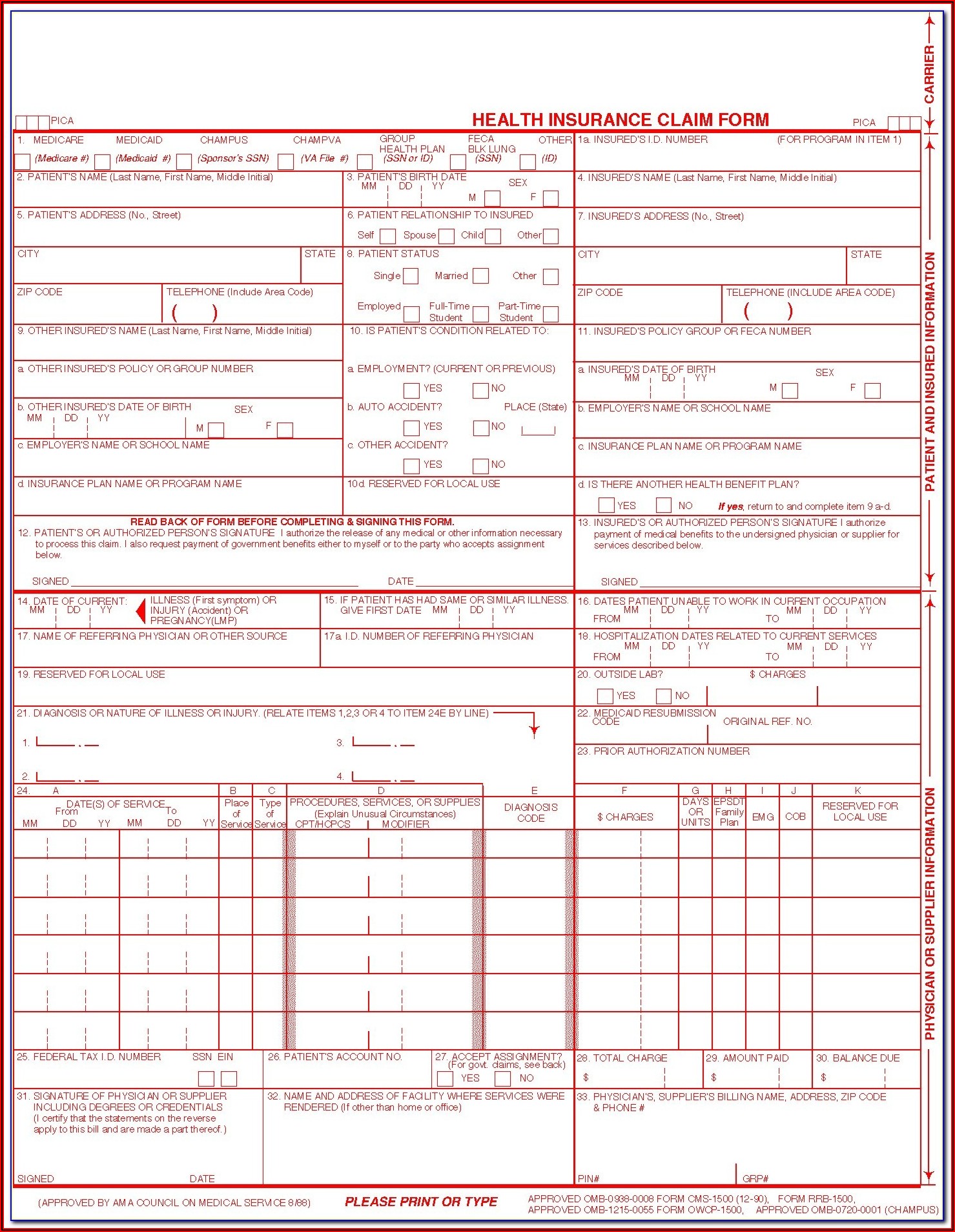
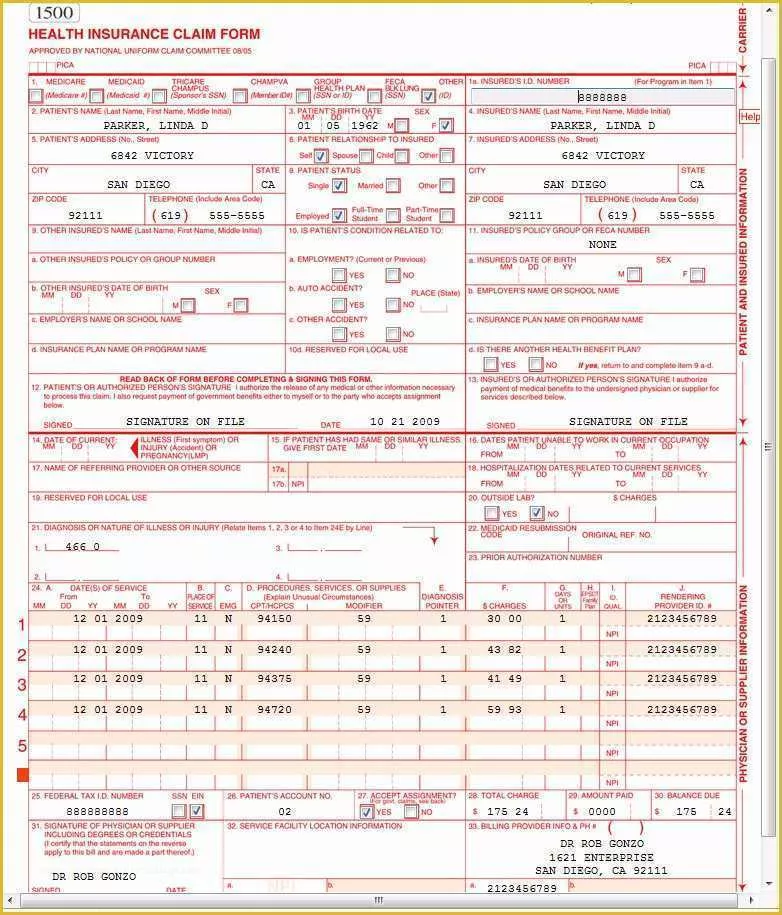
Sign up to get the latest information about your choice of cms topics. It is also used for submitting claims to many private payers and medicaid programs. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete. Last updated wed, 04 jan 2023 13:36:02 +0000 Web the nucc does not process claims. Medicare medicaid champus champva other read back of form before completing & signing this form. Web health insurance claim form 1. Web sample 1500 health insurance claim form for durable medical equipment x 1234567890 member, im a. The form is used by physicians and allied health professionals to submit claims for medical services. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health
When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. In the original reference number space, enter the original claim id. All items must be completed unless otherwise noted in these instructions. • your current forms supplier; Billing info > billing preferences > insurance. To receive copies of the 02/12 1500 claim form, contact: Web health insurance claim form 1. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The nucc does not process claims. • version 11.0 7/23 1500 instruction manual.
Free Printable 1500 Claim Form 02 12 Form Resume Examples XnDEYl0DWl
The nucc does not process claims. Web health insurance claim form 1. Send completed forms to the appropriate payer. In the original reference number space, enter the original claim id. Web the nucc does not process claims.

Free Hcfa 1500 Claim Form Template Form Resume Examples Dp3OOgO30Q
When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. In the original reference number space, enter the original claim id. You may also click in any field for more detailed instructions. Last updated wed, 04 jan 2023 13:36:02 +0000 Send completed forms to the appropriate payer.
Fillable 1500 Claim Form Free Form Resume Examples l6YNvp3Y3z
Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health The nucc does not process claims. Web sample 1500 health insurance claim.
Free Health Insurance Claim form 1500 Template Of Medical Claim form
Web using cms form 1500/hcfa: Item 1a insured’s id number (patient’s medicare health insurance claim number. Web cms 1500 dynamic list information. Billing info > billing preferences > insurance. Send completed forms to the appropriate payer.
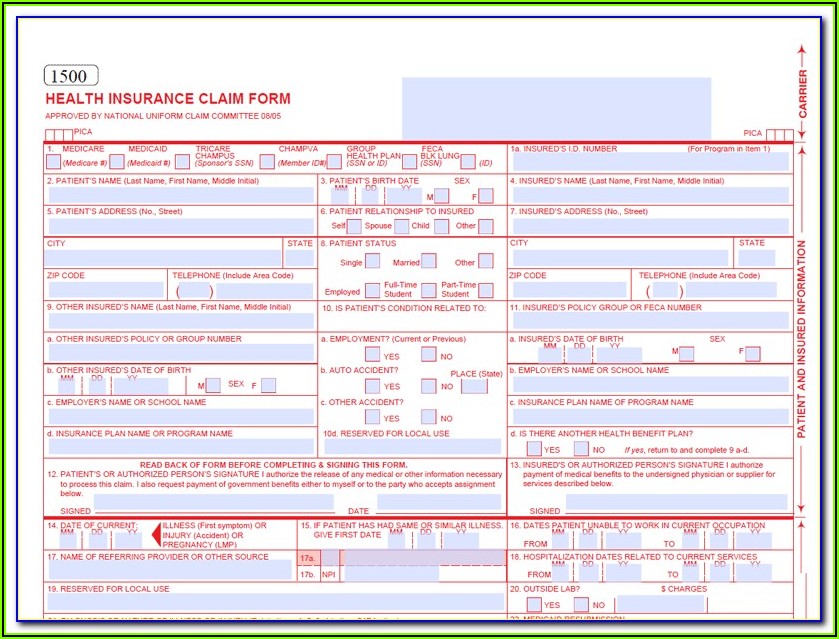
Free Fillable Cms 1500 Claim Form Form Resume Examples emVKNdnYrX
Web the current version of the instructions for the 02/12 1500 claim form was released in july 2022. Web health insurance claim form 1. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health To receive copies of.

Custom CMS 1500 Form Personalized Printed Claim Form CMS 1500 Imprinted
Last updated wed, 04 jan 2023 13:36:02 +0000 It is also used for submitting claims to many private payers and medicaid programs. The form is used by physicians and allied health professionals to submit claims for medical services. You may also click in any field for more detailed instructions. To receive copies of the 02/12 1500 claim form, contact:
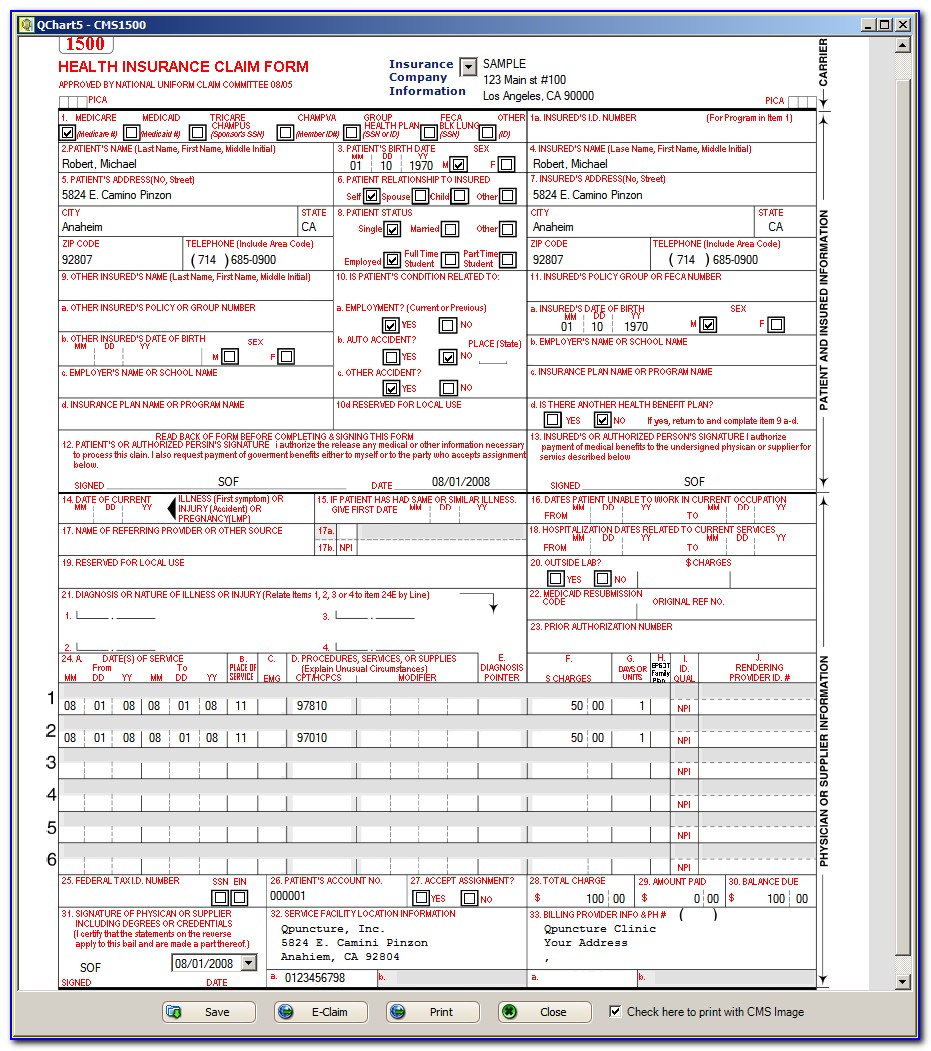
Sample 1500 Claim Form Filled Out Form Resume Examples a15qXrADeQ
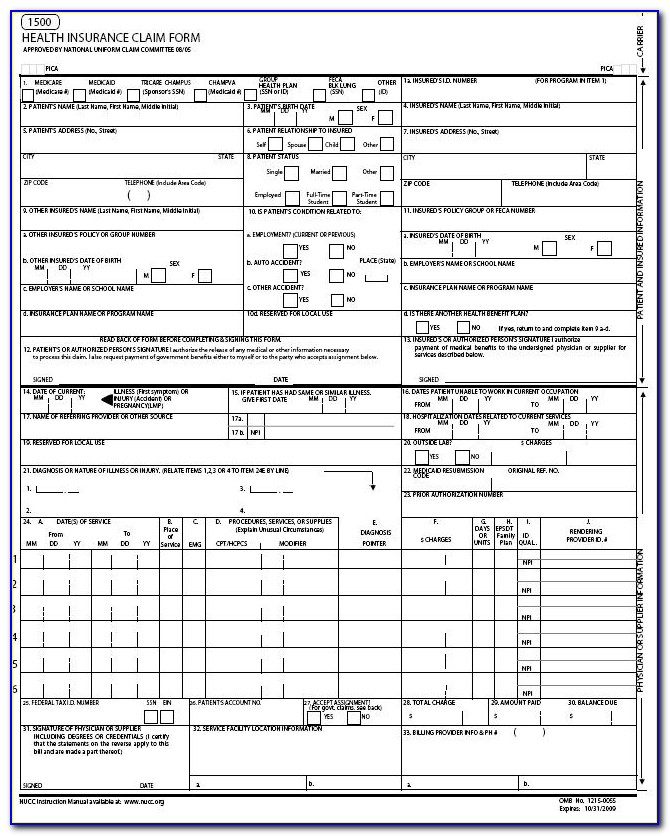
You can decide how often to. Send completed forms to the appropriate payer. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,. Enter the correct frequency code. Last updated wed, 04 jan 2023 13:36:02 +0000
Sample Of New Hcfa 1500 Claim Form Form Resume Examples YL5zpEekzV
In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,. Send completed forms to the appropriate payer. Please.

Insurance Claim Form 1500
Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Item 1a insured’s id number (patient’s medicare health insurance claim number. Web the current version of the instructions for the 02/12 1500 claim form was released in july 2022. You may also click in any field for more detailed instructions. Last updated.

1500 Claim Form Template SampleTemplatess SampleTemplatess
Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. You can decide how often to. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Enter the correct frequency code. • version 11.0 7/23 1500 instruction manual.
Web Using Cms Form 1500/Hcfa:
Web health insurance claim form 1. Web cms 1500 dynamic list information. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,. This form is the only version accepted by medicare.
Failure To Follow These Guidelines Could Cause A Delay In Processing, Denial Of The Claim, Or Affect Payment Accuracy.
Enter the correct frequency code. Last updated wed, 04 jan 2023 13:36:02 +0000 Please mail them to the name and address listed here. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete.
The Form Is Used By Physicians And Allied Health Professionals To Submit Claims For Medical Services.
All items must be completed unless otherwise noted in these instructions. Item 1a insured’s id number (patient’s medicare health insurance claim number. • version 11.0 7/23 1500 instruction manual. It is also used for submitting claims to many private payers and medicaid programs.
Send Completed Forms To The Appropriate Payer.
To receive copies of the 02/12 1500 claim form, contact: Web sample 1500 health insurance claim form for durable medical equipment x 1234567890 member, im a. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services.