Form 3008 Florida Medicaid
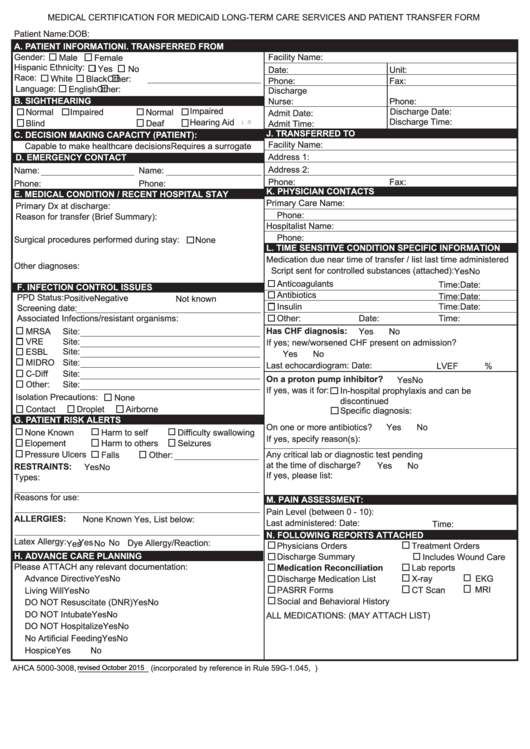
Form 3008 Florida Medicaid - This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. Effective date of medical condition physician/arnp signature: • for the purposes of determining whether an individual meets the medical eligibility criteria, the comprehensive *data required for medicaid if hospitalized: Enjoy smart fillable fields and interactivity. Web how to fill out and sign ahca form 5000 3008 online? Get your online template and fill it in using progressive features. For patients entering a skilled nursing facility: Printed physician/arnp name & title:
*data required for medicaid if hospitalized: Effective date of medical condition physician/arnp signature: Enjoy smart fillable fields and interactivity. Both pages of this form must be completed. Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. Printed physician/arnp name & title: • for the purposes of determining whether an individual meets the medical eligibility criteria, the comprehensive Web how to fill out and sign ahca form 5000 3008 online? For patients entering a skilled nursing facility: This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse.
• for the purposes of determining whether an individual meets the medical eligibility criteria, the comprehensive Get your online template and fill it in using progressive features. This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Web how to fill out and sign ahca form 5000 3008 online? *data required for medicaid if hospitalized: Enjoy smart fillable fields and interactivity. Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. Printed physician/arnp name & title: Follow the simple instructions below: For patients entering a skilled nursing facility:
Florida Medicaid Forms For Providers Form Resume Examples mx2WQzbRY6
Effective date of medical condition physician/arnp signature: Follow the simple instructions below: For patients entering a skilled nursing facility: *data required for medicaid if hospitalized: Printed physician/arnp name & title:
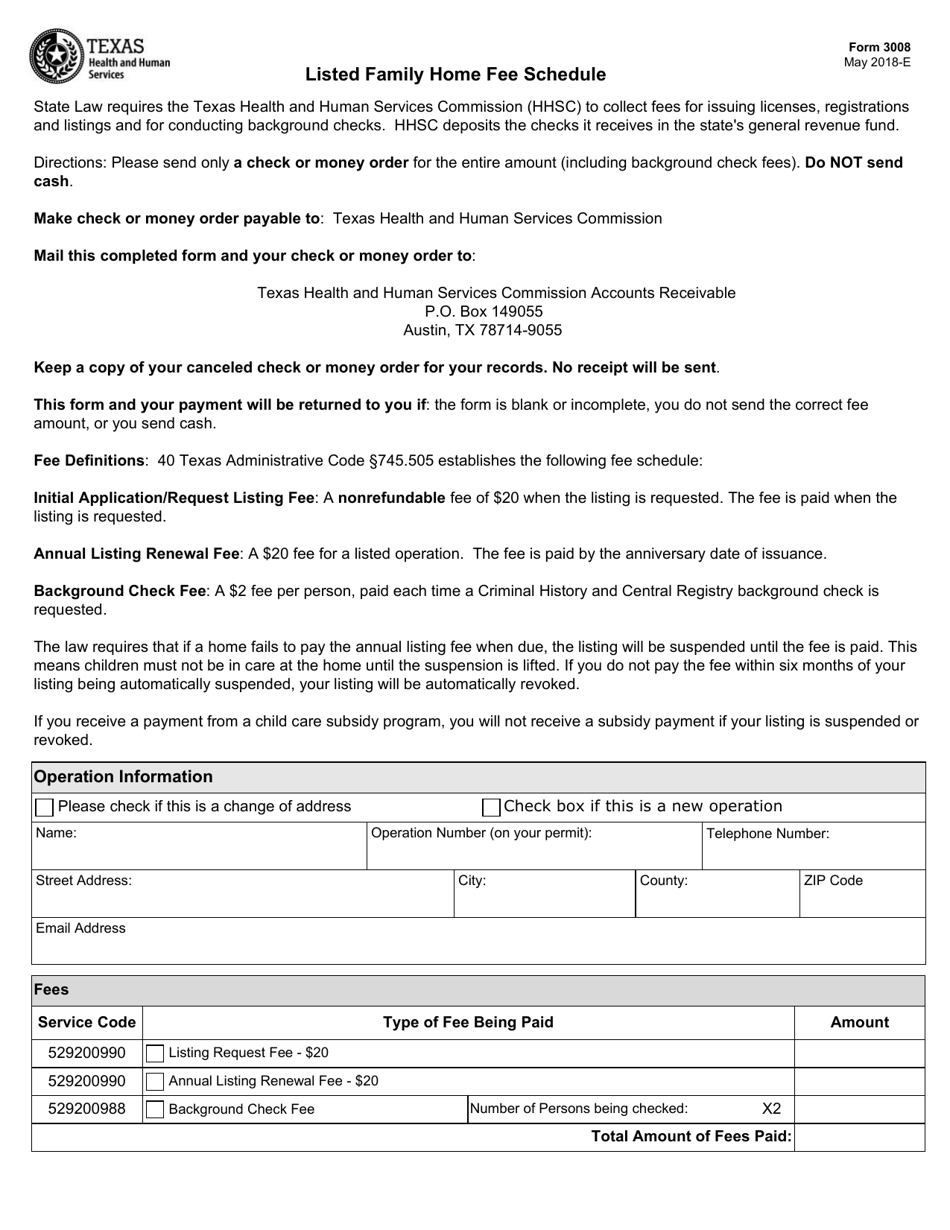
Form 3008 Download Fillable PDF or Fill Online Listed Family Home Fee
Effective date of medical condition physician/arnp signature: This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Enjoy smart fillable fields and interactivity. Printed physician/arnp name & title: Both pages of this form must be completed.
ACHA Form 50003008 Download Fillable PDF or Fill Online Medical
For patients entering a skilled nursing facility: This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Enjoy smart fillable fields and interactivity. Printed physician/arnp name & title: Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement.
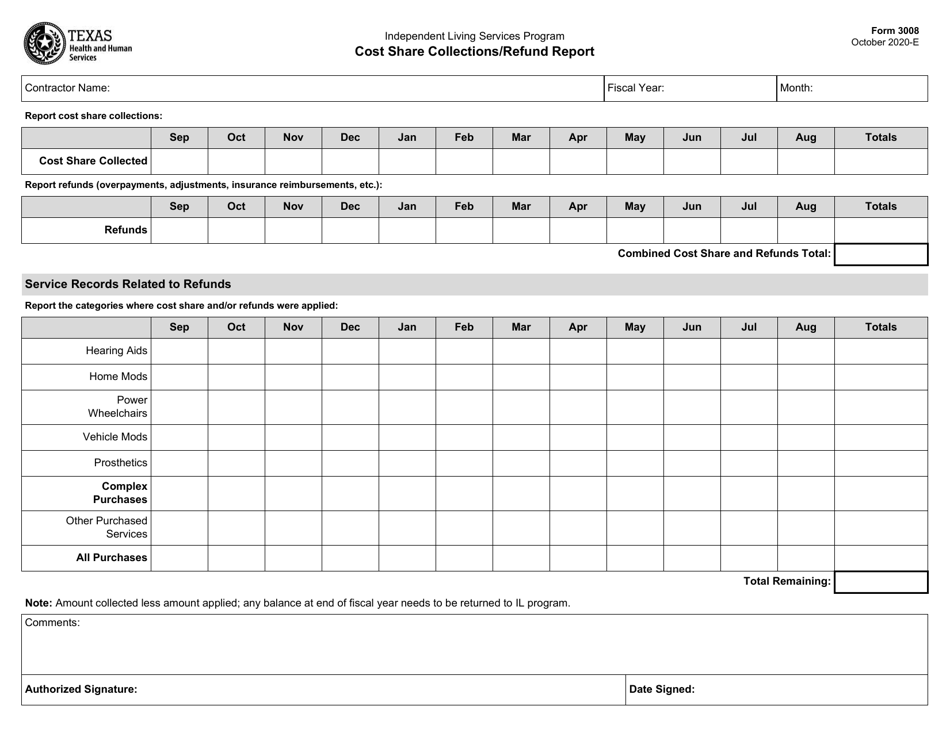
Form 3008 Download Fillable PDF or Fill Online Cost Share Collections
Enjoy smart fillable fields and interactivity. Printed physician/arnp name & title: Get your online template and fill it in using progressive features. This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Follow the simple instructions below:

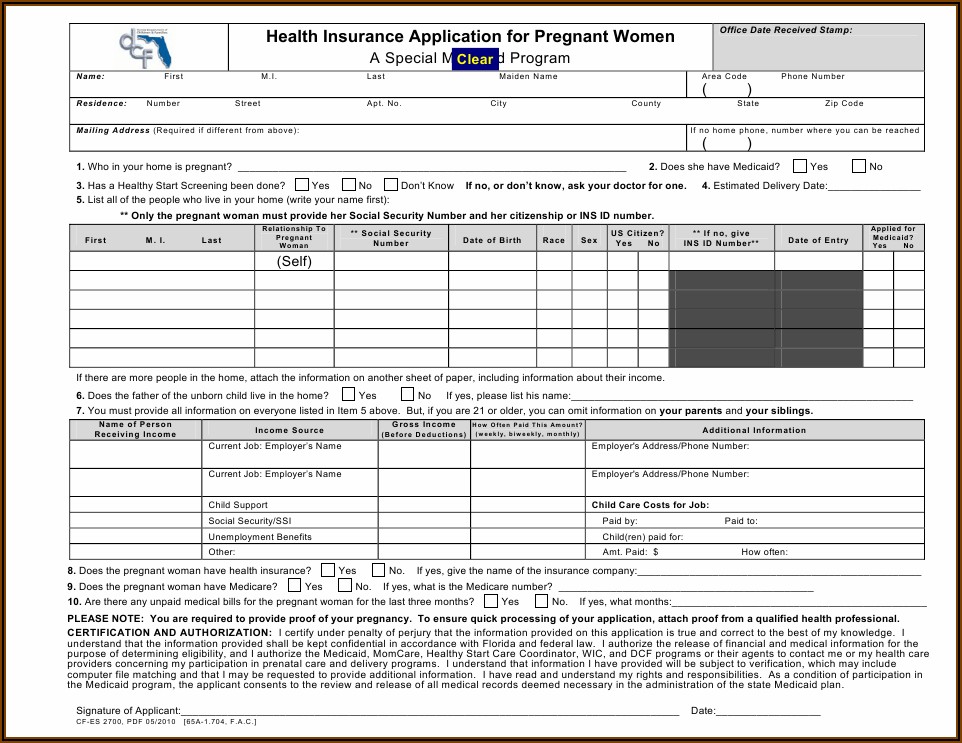
Medicaid Application Form Florida Form Resume Examples
*data required for medicaid if hospitalized: Printed physician/arnp name & title: Get your online template and fill it in using progressive features. Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. Enjoy smart fillable fields and interactivity.

Florida Health Care Surrogate Form
For patients entering a skilled nursing facility: Both pages of this form must be completed. Get your online template and fill it in using progressive features. Effective date of medical condition physician/arnp signature: • for the purposes of determining whether an individual meets the medical eligibility criteria, the comprehensive
Fillable Form Ahca 50003008 Medical Certification For Medicaid Long
Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. Enjoy smart fillable fields and interactivity. Follow the simple instructions below: *data required for medicaid if hospitalized: Effective date of medical condition physician/arnp signature:
Florida Medicaid Tax Forms Form Resume Examples X42M4bMAVk
Enjoy smart fillable fields and interactivity. Get your online template and fill it in using progressive features. Effective date of medical condition physician/arnp signature: *data required for medicaid if hospitalized: Both pages of this form must be completed.
Top 3008 Form Templates free to download in PDF format
Both pages of this form must be completed. This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. Web how to fill out and sign ahca form 5000 3008 online? For patients entering a skilled nursing facility: Effective date of medical condition physician/arnp signature:
Acha 3008 Nursing Home Form essentially.cyou 2022
Both pages of this form must be completed. Enjoy smart fillable fields and interactivity. Web i certify the individual is in need of medicaid waiver services in lieu of nursing facility placement. *data required for medicaid if hospitalized: • for the purposes of determining whether an individual meets the medical eligibility criteria, the comprehensive
• For The Purposes Of Determining Whether An Individual Meets The Medical Eligibility Criteria, The Comprehensive
*data required for medicaid if hospitalized: This form must be signed by a licensed physician, physician assistant, or advanced practice registered nurse. For patients entering a skilled nursing facility: Web how to fill out and sign ahca form 5000 3008 online?
Web I Certify The Individual Is In Need Of Medicaid Waiver Services In Lieu Of Nursing Facility Placement.
Both pages of this form must be completed. Enjoy smart fillable fields and interactivity. Printed physician/arnp name & title: Get your online template and fill it in using progressive features.
Follow The Simple Instructions Below:
Effective date of medical condition physician/arnp signature: